

Summary
The appropriateness of the new American College of Cardiology/American Heart Association (ACC/AHA) “Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults” for patients with diabetes was reviewed in this article [Stone NJ et al. Circulation 2014; J Am Coll Cardiol 2014].
- Diabetes & Endocrinology Guidelines
- Cardiology Guidelines
- Lipid Disorders
- Diabetes Mellitus
- Diabetes & Endocrinology Guidelines
- Cardiology Guidelines
- Lipid Disorders
- Diabetes Mellitus
- Endocrinology
- Diabetes & Metabolic Syndrome
The appropriateness of the new American College of Cardiology/American Heart Association (ACC/AHA) “Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults” for patients with diabetes was reviewed in this session [Stone NJ et al. Circulation 2014; J Am Coll Cardiol 2014].
Arguing in favor of the use of the ACC/AHA guideline to make treatment decisions for patients with diabetes was Robert H. Eckel, MD, University of Colorado Anschutz Medical Campus, Aurora, Colorado, USA. The new guideline reflects the knowledge that vigilant diabetes care has been beneficial, he said, with diabetes-related complications declining from 1995 to 2010, including acute myocardial infarction, stroke, and limb amputation [Gregg EW et al. N Engl J Med 2014].
Similarities between the 2013 ACC/AHA guideline and the one that it replaces (National Cholesterol Education Program Adult Treatment Panel III [ATP III]) are the emphasis on lifestyle, the focus on low-density lipoprotein cholesterol (LDL-C) and the patients at highest risk, and the preference for statins for lipid-lowering therapy.
The greater emphasis on statin use in the 2013 ACC/AHA guideline compared with ATP III is appropriate, stated Dr. Eckel. Statin therapy clearly produces benefits in patients diagnosed with clinical atherosclerotic cardiovascular disease (ASCVD) and those ≥ ≥ 21 years of age with LDL-C ≥ 190 mg/dL (> 4.91 mmol/L). Furthermore, statins are a primary therapy for patients with and without diabetes who are at risk of ASCVD, and they are recommended for 4 benefit groups (Table 1).
Four Statin Benefit Groups in the 2013 ACC/AHA Guideline for Blood Cholesterol
A meta-analysis of 26 randomized controlled trials (RCTs) involving some 170,000 patients showed a reduction of 22% in major vascular events per 1.0-mmol/L reduction in LDL-C from baseline (rate ratio [RR], 0.78; 95% CI, 0.76 to 0.80; p< .0001) [Cholesterol Treatment Trialists' Collaboration. Lancet 2010]. Another meta-analysis by these investigators of 18,686 patients with type 2 diabetes mellitus (T2DM) showed that for each 1-mmol/L reduction in LDL-C, there were similar reductions in major vascular events (RR, 0.79; 95% CI, 0.72 to 0.86; p< .0001), stroke (RR, 0.79; 95% CI, 0.67 to 0.93; p = .0002), coronary revascularization (RR, 0.75; 95% CI, 0.64 to 0.88; p< .0001), and all-cause mortality (RR, 0.91; 95% CI, 0.82 to 1.01; p = .02) [Cholesterol Treatment Trialists' Collaborators. Lancet 2008].
The ACC/AHA guideline reflects the strong evidence that statin therapy at the appropriate intensity is of value to reduce the risk of ASCVD in patients with or without diabetes, stated Dr. Eckel. The lack of targets for LDL-C and non—high-density lipoprotein cholesterol (non-HDL-C) is that there was no RCT evidence to support this. The guideline provides quantitative comparisons of the risk-benefit ratio with statins. Nonstatin therapies were not included in the guideline, because there is no evidence to support a reduction in ASCVD or a safety profile comparable with that of statins.
Additional factors that are useful to make treatment decisions for patients who do not clearly fall into 1 of the 4 statin benefit groups are family history of premature ASCVD, higher lifetime risk of ASCVD, elevated LDL-C (≥ 160 mg/dL [4.13 mmol/L]), elevated high-sensitivity C-reactive protein (≥ 2.0 mg/dL), and presence of subclinical atherosclerosis. Nonetheless, major issues remain: the validation of the risk estimator that is based on the diverse population in the National Health and Nutrition Examination Survey and provides lifetime and 10-year risk; the threshold of ≥ 7.5% 10-year cardiovascular (CV) disease risk to initiate statins for primary prevention; no target levels for LDL-C or non-HDL-C; and potential bias within the guideline-writing committee.
Dr. Eckel emphasized that the 2013 ACC/AHA guideline is meant to guide, not dictate, treatment decisions, and it can and should be used to treat patients with diabetes.
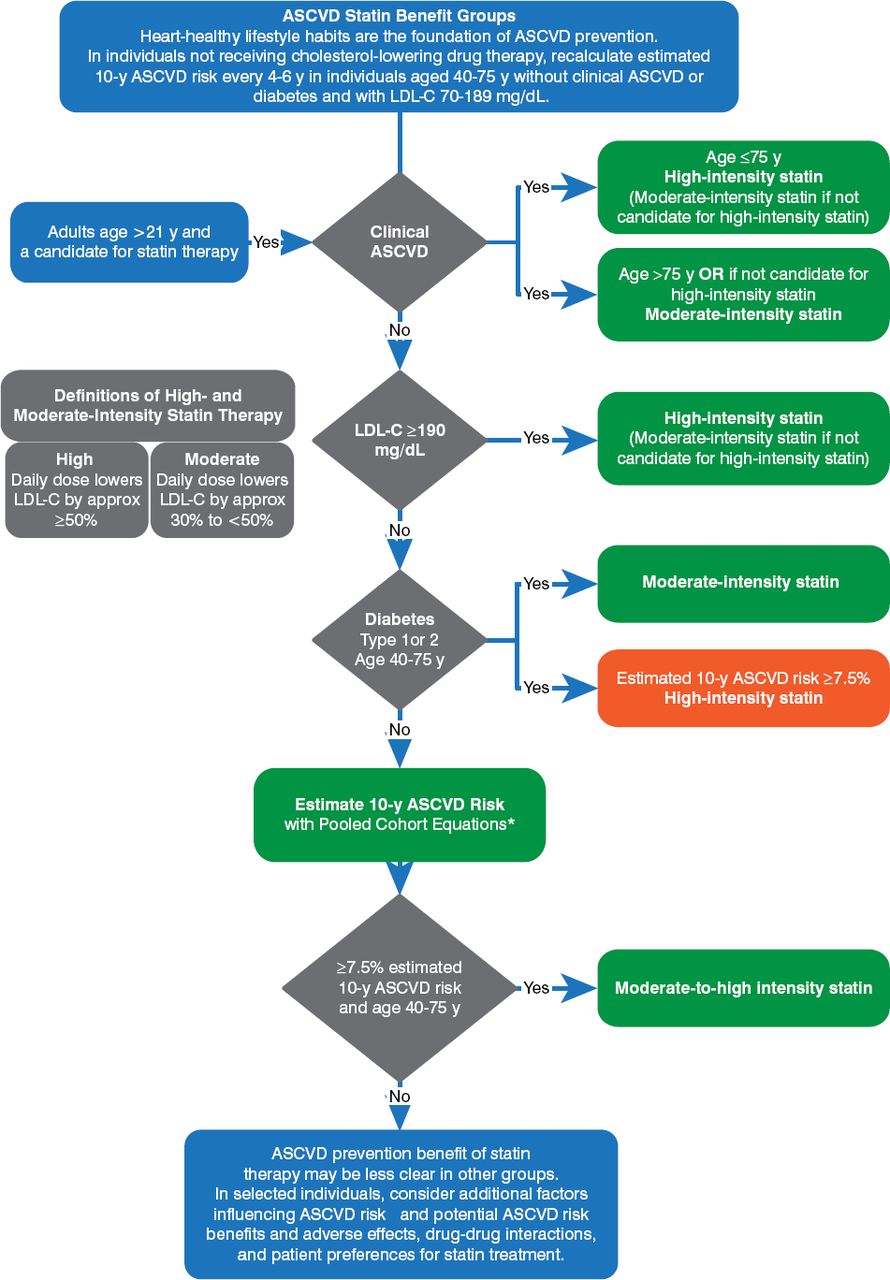
Henry N. Ginsberg, MD, Columbia University College of Physicians and Surgeons, New York City, New York, USA, argued against the use of the 2013 ACC/AHA guideline for patients with diabetes. The major treatment recommendations from this guideline for statins to prevent ASCVD are presented in Figure 1.

Major Recommendations for Statin Therapy for Prevention of Atherosclerotic Cardiovascular Disease
ASCVD = atherosclerotic cardiovascular disease; LDL = low-density lipoprotein; y = year.
Reproduced from Stone NJ et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(suppl 2):S1-S45. With permission from Lippincott Williams and Wilkins.
The key point is whether the 2013 ACC/AHA guideline is strictly evidence based. The recommended treatment is a high-intensity statin for patients with and without diabetes. However, there is a caveat that there is no evidence from RCTs in patients with low LDL-C levels at baseline or in the very young or very elderly. Moreover, the treatment recommendations for patients with LDL-C ≥ 190 mg/dL were based on consensus and expert opinion. Furthermore, some RCT data have favored the use of moderate-intensity statins for T2DM [Auer J et al. Lancet 2004], and the limited data for type 1 diabetes are from a meta-analysis (1466 of 18 686 patients) [Lancet 2008]. It is arguable, therefore, whether or not the ACC/AHA guideline is strictly evidence based, stated Dr. Ginsberg.
Diabetes increases CV mortality compared with patients without diabetes, with a linear increase in risk as the number of risk factors increase (smoking, dyslipidemia, hypertension). The greater efficacy of atorvastatin at 80 mg compared with 10 mg in lowering LDL-C in high-risk patients was associated with greater reductions in the cumulative incidence of a first major CV event, nonfatal myocardial infarction, and death from coronary heart disease (CHD) [LaRosa JC et al. N Engl J Med 2005]. Additionally, the efficacy of atorvastatin at 80 mg versus pravastatin at 40 mg in reducing both LDL-C and death due to a major CV event has been shown [Cannon CP et al. N Engl J Med 2004]. These and 2 other similar trials have shown that greater reductions of LDL-C are associated with greater reductions in CHD events; therefore, there should be goals for LDL-C, such as those in ATP III or the 2006 ACC/AHA guidelines. Use of nonstatin drugs to achieve those goals, if statin monotherapy fails to do so, seems reasonable and could have been offered as consensus or expert opinion.
Regarding the threshold of ≥ 7.5% 10-year CV disease risk for people without diabetes or ASCVD, Dr. Ginsberg stated that no RCTs have randomly assigned patients by baseline risk and there are no RCT data to support this recommendation.
The American Diabetes Association recommendations for treating lipids are better than the ACC/AHA guidelines for patients with diabetes, stated Dr. Ginsberg [American Diabetes Association. Diabetes Care 2013]. Its key recommendations are summarized in Table 2.
American Diabetes Association Lipid Guidelines: Recommendations for Patients With Diabetes
Dr. Ginsberg stated that the ACC/AHA guideline should have provided recommendations for treatment with agents other than statins when LDL-C is > 70 mg/dL in patients who have CVD or are at very high risk. Also, the goals for total cholesterol and HDL-C should include diet and exercise, with nonstatin combination therapy considered for more severe dyslipidemia.
In summary, Dr. Ginsberg supported the identification of 4 groups of patients who, according to their high risk for CVD, deserved treatment with statins. However, he questioned 3 aspects of the 2013 ACC/AHA guideline regarding the treatment of individuals in those 4 groups. First, previous guidelines had targets for LDL-C, while the new guideline advocates statin treatment with no regard for the ultimate LDL-C level. Second, previous guidelines linked statin intensity and LDL-C cutoffs and targets, while the latest guideline eliminates these yet still recommends different levels of statin intensity. Third, prior guidelines had no age-related cutoffs, while the current guideline has an upper limit of 75 years for its main recommendations.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.