

Summary
At the time of the session, the ongoing Ebola outbreak in West Africa had killed nearly 4500 people, including more than 200 health care workers, likely an underestimate of the actual numbers. In a worst-case scenario, the World Health Organization and US Centers for Disease Control and Prevention estimate that the number of cases could reach almost
1.5 million by early 2015. This article discusses infection control in dentistry. At the time of the session, the ongoing Ebola outbreak in West Africa had killed nearly 4500 people, including more than 200 health care workers, likely an underestimate of the actual numbers. In a worst-case scenario, the World Health Organization and US Centers for Disease Control and Prevention estimate that the number of cases could reach almost
1.5 million by early 2015. This article discusses infection control in dentistry. At the time of the session, the ongoing Ebola outbreak in West Africa had killed nearly 4500 people, including more than 200 health care workers, likely an underestimate of the actual numbers. In a worst-case scenario, the World Health Organization and US Centers for Disease Control and Prevention estimate that the number of cases could reach almost
1.5 million by early 2015. This article discusses infection control in dentistry. At the time of the session, the ongoing Ebola outbreak in West Africa had killed nearly 4500 people, including more than 200 health care workers, likely an underestimate of the actual numbers. In a worst-case scenario, the World Health Organization and US Centers for Disease Control and Prevention estimate that the number of cases could reach almost
1.5 million by early 2015. This article discusses infection control in dentistry. At the time of the session, the ongoing Ebola outbreak in West Africa had killed nearly 4500 people, including more than 200 health care workers, likely an underestimate of the actual numbers. In a worst-case scenario, the World Health Organization and US Centers for Disease Control and Prevention estimate that the number of cases could reach almost
1.5 million by early 2015. This article discusses infection control in dentistry. At the time of the session, the ongoing Ebola outbreak in West Africa had killed nearly 4500 people, including more than 200 health care workers, likely an underestimate of the actual numbers. In a worst-case scenario, the World Health Organization and US Centers for Disease Control and Prevention estimate that the number of cases could reach almost
1.5 million by early 2015. This article discusses infection control in dentistry.
- Preventive & Public Health Viral Infections
- Infection Control
- Preventive & Public Health Dentistry
- Viral Infections
- Infection Control
- Dentistry
John Molinari, PhD, The Dental Advisor, Ann Arbor, Michigan, USA, discussed infection control in dentistry. At the time of the talk, the ongoing Ebola outbreak in West Africa had killed nearly 4500 people, including more than 200 health care workers, likely an underestimate of the actual numbers. In a worst–case scenario, the World Health Organization and US Centers for Disease Control and Prevention estimate that the number of cases could reach almost 1.5 million by early 2015.
Closer to home, 2 cases of Ebola infection (the first involving a nurse, with another nurse becoming ill the following week) were active within 300 miles of the conference site. Given the previous rarity of this infection in the United States and the concerns among health care staff, including dentists and dental hygienists, about the possibilities of viral transmission in infected but as yet asymptomatic patients, Ebola was the launching point of Dr Molinari's talk.
Ebola is one of several known filovirus types that cause illness in humans. The natural reservoir of Ebola is undetermined but may be the fruit bat. The pattern of transmission of Ebola in the natural host is also unknown, and the spread to humans is unclear. Once humans are infected, an outbreak involves person–to–person transmission through blood and body fluids that include urine, feces, saliva, vomit, sweat, and semen. Infection can occur when virus–laden fluid comes into contact with broken skin; absorption through mucous membranes also occurs. If an inanimate object is wet from the blood or fluid of a contaminated person, for example, transmission can occur if someone else touches the object and then transfers his or her hand to the mouth or rubs a cut, because the virus can remain capable of infection when outside of the body for days, perhaps weeks.
A person who is infected may not display symptoms for 8 to 10 days, with some people remaining asymptomatic for up to 3 weeks. Fever, headache, and muscle pain then develop abruptly. Initially, the infection can be mistaken for influenza. In up to half of those infected, however, internal bleeding as well as bleeding from mucous membranes in the nose, gastrointestinal tract, vagina, and gums can occur. With these later manifestations, the subsequent outlook is grim, with a death rate that varies from 25% to 90% depending on the type of infecting virus. The average death rate is about 50%.
In addition to copious bleeding, these later events include bruising, small round spots on the skin due to hemorrhage of capillaries, accumulation of fluid around the lungs, shock, and kidney failure. Laboratory findings include leukopenia or leukocytosis, thrombocytopenia, indications of liver damage, anemia, and prolonged prothrombin time and partial thromboplastin time.
The infection is not spread by inhalation. Transmission requires person–to–person spread through direct contact with body fluid. Of relevance to dentistry, this would include aerosolized fluids from the mouth and contact with blood during dental procedures such as a tooth extraction.
Dealing with a person with a confirmed or suspected Ebola infection requires isolation of the patient from other patients and strict safety precautions by health care workers that include use of a respirator (at least as protective as an N95 respirator), a surgical mask, a fluid–resistant or impermeable gown, leg and shoe coverings, double gloves to prevent access of fluid through pinprick holes, and a full face shield or goggles. The gloves and shoe covers are typically taped to the gown to prevent access of fluid to the underlying skin. Where possible, patients should be housed in a negative–pressure room with vented air filtered through a high–efficiency particulate air filter. Ideally, the personal protective equipment is discarded after use. In the resource–challenged conditions of the African outbreak, however, boots and gloves are reused after disinfection with 0.5% bleach and exposure to sunlight (ultraviolet exposure). Scrupulous hand hygiene using soap and water or an alcohol–based hand rub is crucial [Kohn WG et al. MMWR. 2003].
Due to a general lack of appropriate equipment in the majority of dental offices, as well as inexperience in dealing directly with the infection, the American Dental Association (ADA) Division of Science suggests that all dental professionals, including dentists and hygienists, avoid treating patients who exhibit the signs and symptoms of Ebola. Capturing a patient's medical history, including recent travel patterns, will help dental professionals assess the level of risk if the infection is suspected. The general consensus from the ADA, however, remains to avoid treating patients who show any indications of having Ebola [ADA Division of Science. Ebola Resources for Dentists. 2014]. Another virus that has garnered recent attention is enterovirus D68. This nonpolio enterovirus is very common, with more than 100 known viral types, and usually causes 10 to 15 million cases of a relatively mild respiratory illness annually. The cold acquired by many people in the summer months is usually due to an enterovirus infection. However, an outbreak of enterovirus D68 during the summer and autumn of 2014 that concentrated in the western and midwestern United States, but is now documented in almost every state, has featured severe respiratory symptoms that include fever, runny nose, runny eyes, cough, muscle ache, skin rash, wheezing, and difficulty breathing. Infants, children, and teenagers are the most susceptible, because they can lack full immunity due to inadequate prior exposure to the virus. Children with asthma are at heightened risk of severe respiratory infection. Extreme consequences are viral meningitis, myocarditis, endocarditis, encephalitis, and paralysis, and 4 deaths have been linked to the infection.
Of relevance to dentists and dental hygienists, D68 can also be spread from person to person in respiratory secretions like saliva, nasal mucus, and sputum. Infection control precautions include frequent hand–washing and disinfection of surfaces in the vicinity of the patients with a disinfectant that has been proven to be efficacious against nonenveloped viruses, such as poliovirus, norovirus, papillomavirus, and hepatitis A virus.
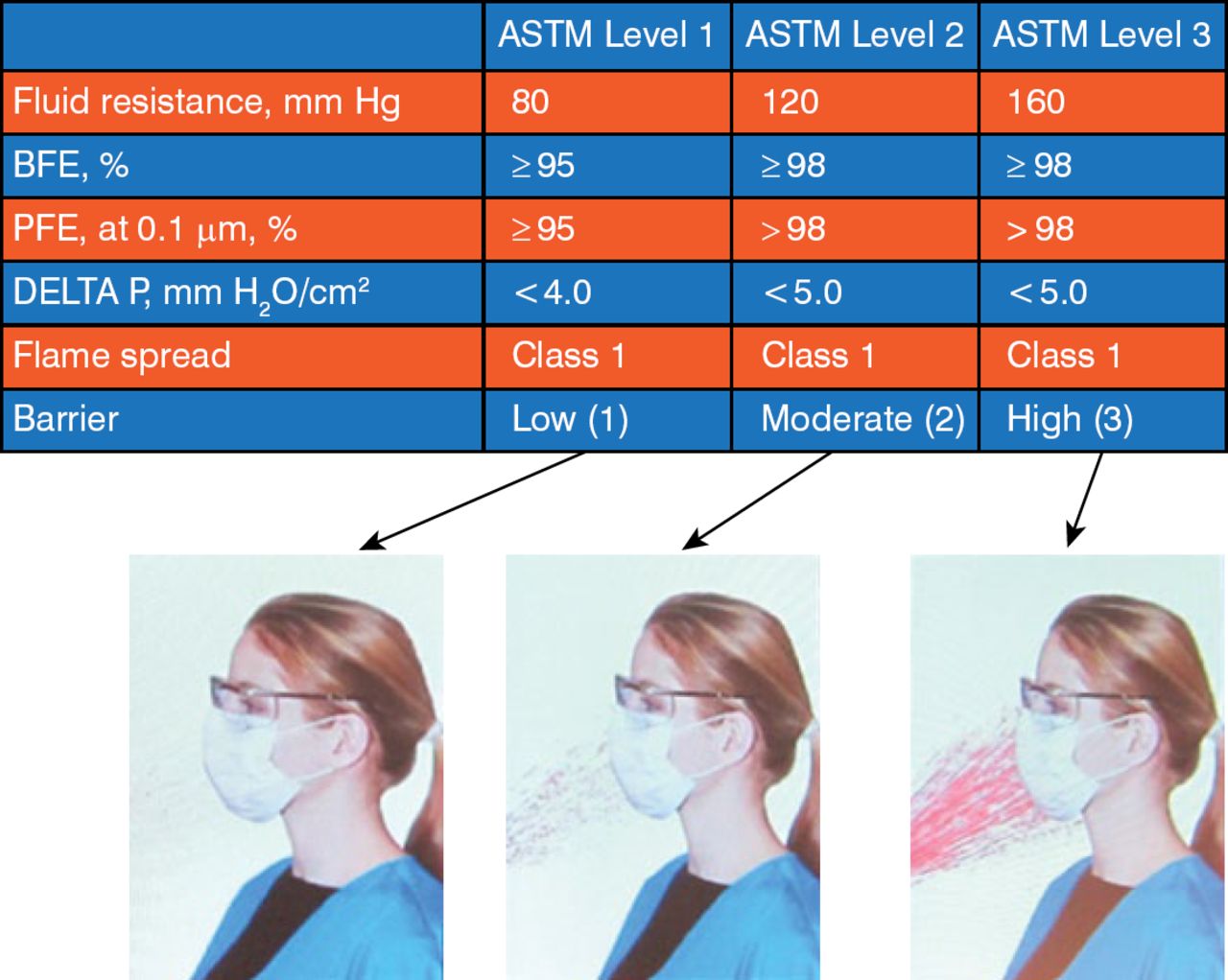
The use of appropriate personal protective equipment (glasses or a face guard, a face mask, and a gown) is required. In a typical dental setting, the generation of aerosols and water droplets can soak a face mask within minutes. If the moisture can be felt through the mask, the chance for transmission of an airborne pathogen exists. In this case, the use of an American Society of Testing and Materials level 1 mask would not be the appropriate choice. Rather, a level 2 or 3 mask would offer the desired protection depending on the assessed risk of exposure (Figure 1).

Different Face Masks for Different Levels of Exposure
ASTM, American Society of Testing and Materials; BFE, bacteria filtration efficiency; DELTA P, differential pressure; PFE, particle filtration efficiency.
Reproduced with permission from J Molinari, PhD.
The reality for the dental profession is the possibility of exposure to microorganisms that have become more pathogenic to humans. Infection control precautions should be enacted with this reality in mind (Figure 2).

The Reality of Dentistry
Reproduced with permission from J Molinari, PhD.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.