

Summary
Oral cancer is a highly destructive disease that is associated with significant morbidity. Surgery with follow-up radiation is the most common treatment but almost always leaves patients with obvious physical changes and functional deficits. Because the size of the tumor determines the extent of the surgery, early diagnosis and intervention offer the best chances to survive and minimize these effects. This article discusses early identification of oral tissue changes that may indicate oral cancer and argued in favor of an ongoing relationship between dentists and oral pathologists as a way of optimizing patient care.
- Head & Neck Cancers
- Pathology
- Head & Neck Cancers
- Pathology
- Dentistry
- Exclusive Article - For home page
Oral cancer is a highly destructive disease that is associated with significant morbidity. Surgery with follow–up radiation is the most common treatment but almost always leaves patients with obvious physical changes and functional deficits. Because the size of the tumor determines the extent of the surgery, early diagnosis and intervention offer the best chances to survive and minimize these effects. John M. Wright, DDS, MS, Texas A&M University, Dallas, Texas, USA, discussed early identification of oral tissue changes that may indicate oral cancer and argued in favor of an ongoing relationship between dentists and oral pathologists as a way of optimizing patient care.
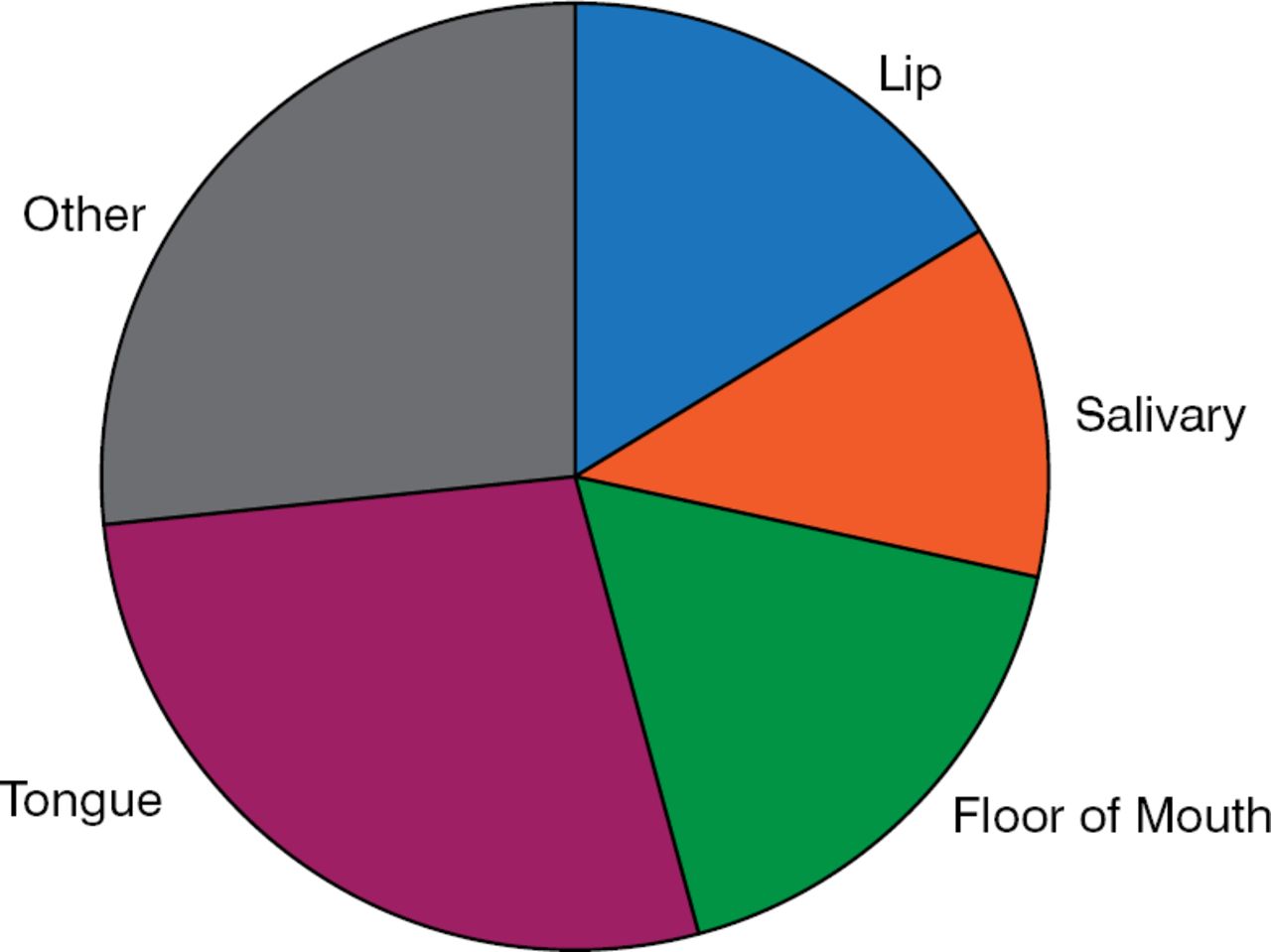
Oral cancer in the United States includes carcinoma of the lip, salivary glands, mouth, and throat, and it accounts for about 1% to 3% of all cancers (Figure 1). For 2014, the American Cancer Society has projected around 42 000 new cases and about 8400 oral cancer–related deaths [American Cancer Society. Cancer Facts and Figures. 2014]. The incidence is increasing among women and younger patients, but for both sexes, the risk increases considerably beginning at about age 45.

Oral Cancer Incidence by Site
Reproduced with permission from JM Wright, DDS, MS.
The most common cancer affecting the structures of the mouth is squamous cell carcinoma (SCC). The most common site is the posterior–lateral tongue. The major risk factors for cancer of the mouth are alcohol and smoking (the relationship between smokeless tobacco and oral cancer is disputed). About 75% of oral–pharyngeal cancer is due to smoking, and the relative risk associated with a combination of smoking and drinking is significantly greater than that of either product alone. Dr Wright believes that the additives in alcoholic beverages, as opposed to the alcohol itself, are responsible for the increased risk, because no direct cause–effect relationship has been demonstrated between pure ethyl alcohol and cancer. Among young women, chronic iron deficiency has also been shown to increase the risk of oral cancer. Recently, a relationship has also been demonstrated between human papilloma virus (HPV), particularly HPV16, and oropharyngeal cancer. HPV–related oropharyngeal cancer represents around 80% of current cases. It is seen predominantly among men and is strongly correlated with sexual practices. Median survival for this form of cancer is considerably longer compared with cancer resulting from other causes (131 months for patients with HPV+ disease vs 20 months for those with HPV–disease). As with other forms of cancer, diets rich in fruits and vegetables have been shown to have a protective effect against oral cancer.
There has been some increase in the 5–year survival rate for patients with oral cancer. Currently, the overall 5–year survival rate is about 60% (Table 1). A major influence on survival is the low rate of early diagnosis. Almost 50% of patients diagnosed with oral cancer are diagnosed only after their cancer has spread to the regional lymph nodes, which significantly and adversely affects survival. Dr Wright believes that clinicians should not only conduct regular oral cancer screenings but also use that as an opportunity to educate their patients on which signs and symptoms the patient should not ignore. The high–risk patient profile and sites for oral cancer are shown in Table 2.
Comparison of 5–Year Survival by TNM and STNMP Classification
High–Risk Profile for Oral Cancer
One area of potential early diagnosis that is often overlooked is failed dental implants. The use of dental implants is widely accepted by both patients and clinicians, and although they are almost always a successful procedure, they do, on occasion, fail. At this time, there is no universally accepted protocol for the treatment of peri–implantitis (PI). The tissue removed during treatment of PI is not routinely submitted for histopathologic examinations, so there is only sparse information on the microscopic findings in these patients. It is important to remember that oral cancer is just as much a possibility with an implant as it is with a normal tooth. Dr Wright also provided results from an unpublished study of 167 peri–implant biopsies from several clinics in Israel; most specimens (almost 40%) were found to have nonspecific inflammation, but 4.2% were found to be malignant. Other results were typical of those found in tissue surrounding normal teeth, and they included pyogenic granuloma (17.4% of cases), giant cell granuloma (5.9%), colonies of Actinomyces surrounded by inflammation (22.7%), and bisphosphonate–related osteonecrosis of the jaw (2.4%). Results of a review of the literature published between 1990 and 2011 identified 18 articles that reported a total of 41 cases of peri–implant malignancy, including 39 cases of SCC and 1 of sarcoma [Moergel M et al. Clin Oral Investig. 2014]. Almost all cases (n = 38) were found in the mandible.
There are several variants of SCC; with the exception of verrucous carcinoma, most are rare. Verrucous carcinoma was first identified in 1948 and was named because of its verrucous surface architecture. It is a relatively low–grade cancer that rarely metastasizes; however, it can grow very large and ranges in color from white to pink. It is often seen in those who chew tobacco or use snuff orally.
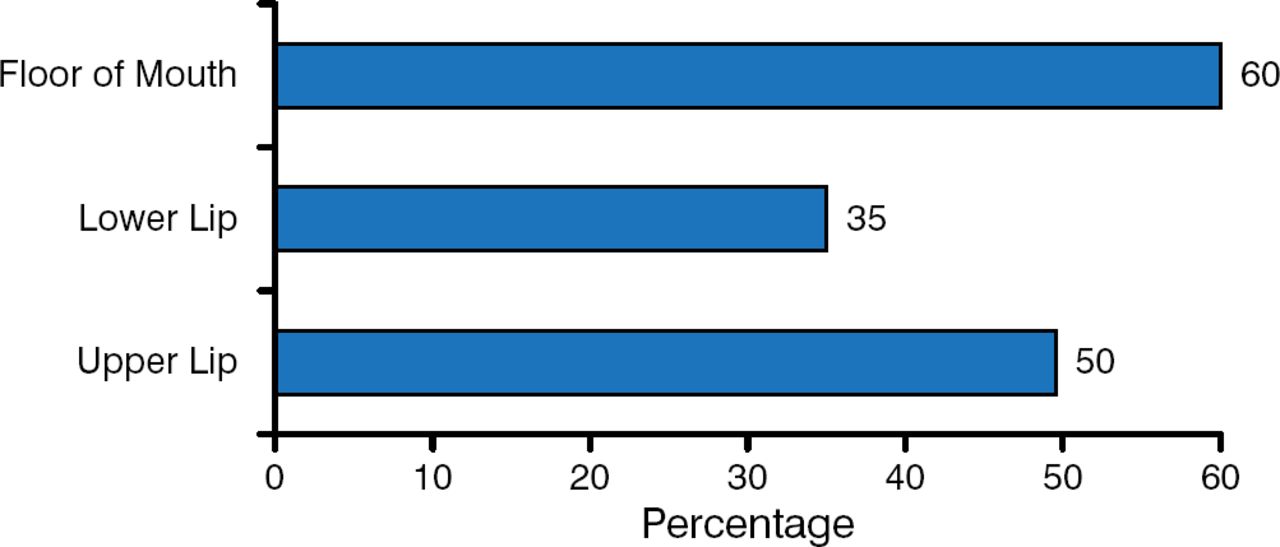
One of the most important characteristics of oral cancer is that it is associated with a premalignant process, which can last for years, during which lesions are clinically detectable. Diagnosis and treatment at this phase can prevent the development of oral cancer. Although most leukoplakia is benign, it is closely associated with the use of tobacco and may be an early sign of cancer. It is important to encourage these patients to quit their tobacco use, because once patients quit, the lesions often resolve. The most accurate measure of whether a leukoplakia will become oral cancer is whether it harbors epithelial dysplasia histologically. Overall, only approximately 20% of leukoplakias, when biopsied, show dysplasia or early invasive carcinoma. Leukoplakias of the floor of the mouth, tongue, and lip are more likely to be dysplastic than those from other areas of the mouth (Figure 2).

Areas at Risk: Percentage of Specimens Showing Dysplasia or Carcinoma
Reproduced with permission from JM Wright, DDS, MS.
The clinical change in a leukoplakia that increases its likelihood of being dysplastic is any area of redness or ulceration or areas that are “bumpy or pebbly”; size is not an indicator. Roughly 1% to 3.5% of patients with nondysplastic leukoplakia lesions will progress to cancer, indicating a need to monitor these patients [Hsue SS et al. J Oral Pathol Med. 2007; Cowan CG et al. Oral Dis. 2001]. Despite complete excision of the lesion, some patients with epithelial dysplasia will still progress to cancer; recurrence is not uncommon [Sperandio M et al. Cancer Prev Res (Phila). 2013; Spielmann PM et al. Eur Arch Otorhinolaryngol. 2010].
Erythroplakias are also premalignant lesions. They are characterized by their red color and at times can be symptomatic (pain and burning). They can be difficult to differentiate from simple inflammation, but once identified, a biopsy is mandatory, because the majority of erythroplakia is dysplastic.
Several diagnostic adjuncts are available, including brush cytology and imaging systems. Although brush cytology has improved sample collection, it does not provide a definitive diagnosis and it cannot detect 80% of premalignant nondysplastic lesions. Only limited evidence for efficacy is available for the imaging systems.
Therapies for oral premalignant lesions may include local and systemic vitamin A and retinoids, systemic β-carotene, lycopene, ketorolac, topical bleomycin, photo–dynamic therapy, blocking EGFR via inhibition of COX–2 and EGFR tyrosine kinase, and gene therapy (particularly p53). It is hoped that, with time, a nonsurgical approach to premalignant oral lesions will be available.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.