

Summary
This article discusses some complications that may be encountered in outpatient dental practice, as well as methods by which to avoid and manage them. Specific highlights include complications in outpatient dental practice are important to consider for various reasons, such as their associated medicolegal implications and potential loss of revenue, and described some of the most common types of complications that can occur.
- Dental Anesthesia
- Surgical Procedures
- Dental Anesthesia
- Surgical Procedures
- Dentistry
In an education course, Mehran Hossaini, DMD, University of California, San Francisco, California, USA, discussed some complications that may be encountered in outpatient dental practice, as well as methods by which to avoid and manage them.
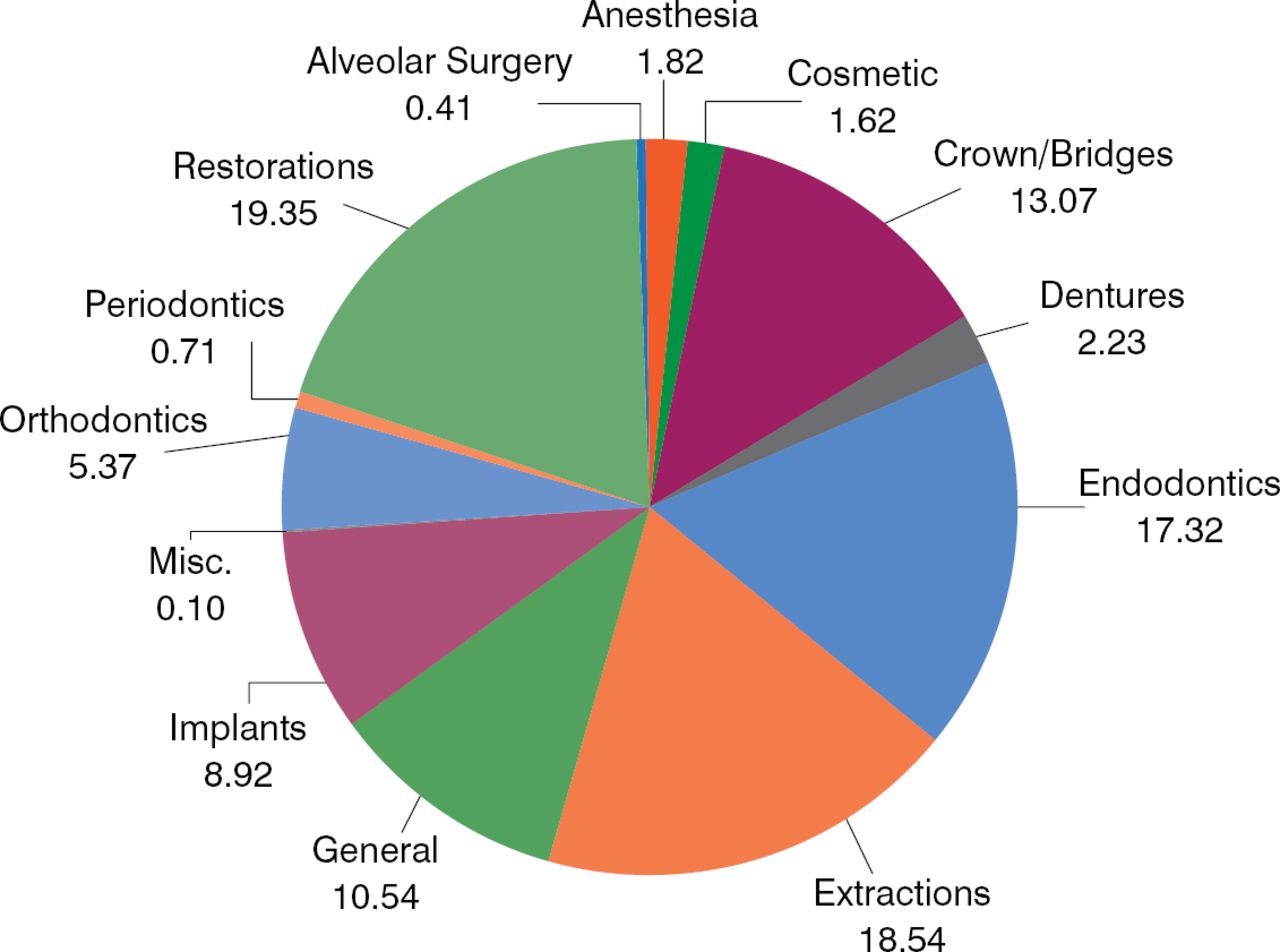
Dr Hossaini highlighted that complications in outpatient dental practice are important to consider for various reasons, such as their associated medicolegal implications (Figure 1) and potential loss of revenue, and described some of the most common types of complications that can occur.

Distribution of Professional Liability Claims in Dental Practice, %
Reproduced with permission from M Hossaini, DMD.
COMPLICATIONS OF LOCAL ANESTHESIA
According to Dr Hossaini, common complications of local anesthesia include the following.
Pain at the injection site: This is typically due to use of a dull needle, rapid injection rate, the presence of inflammation, or poor injection technique. To avoid this complication, Dr Hossaini emphasized the need to pay attention to technique, particularly replacing the needle after multiple uses.
Hematoma formation, infection, or trismus: These 3 issues can also arise from the use of dull, damaged, or contaminated needles as well as from vascular damage or bleeding disorders in patients. Affected patients may require aggressive physical therapy, anti–inflammatory medication, warm compresses, and antibiotic therapy. Muscle relaxants may also be helpful, and patients should be advised to eat a soft diet.
Discussing the problem of trismus, Dr Hossaini stressed the need to attempt forced opening of the jaw to determine whether there is true restriction of movement or whether it is a guarding mechanism due to pain.
Nerve damage: Because of reporting issues, it is difficult to precisely ascertain the incidence of nerve damage following inferior alveolar local anesthesia; Dr Hossaini stated that extrapolated data show approximately 1 in 20 000 to 850 000 patients, with the lingual nerve affected in 70% of cases.
Although it remains unknown why local anesthesia causes nerve damage, mechanisms such as direct trauma, neurotoxicity, and hemorrhage have been proposed. Medical management of the pain should be considered in these patients, because many respond well to gabapentin therapy. Antidepressant medication may also be helpful, particularly with tricyclic antidepressants or serotonin– or norepinephrine–reuptake inhibitors.
Broken needle: Rarely, a needle may break during injection of the local anesthetic (LA). Typically, this may result from use of a 30–gauge needle, use of a bent needle, insertion of the needle to the hub, or multiple use of the same needle. Affected patients require surgical management to remove the needle. This problem, however, is preventable, and actions should be taken to avoid its occurrence, including modification of the needle type used and needle handling.
Other complications: These include toxicity, reaction to vasoconstrictor, syncope, allergic reaction, and missed nerve blocks or inadequate anesthesia.
COMPLICATIONS OF EXTRACTION
Complications associated with tooth extraction include the following.
Tooth or implant displacement: Common sites for tooth or implant displacement include the sinus, infratemporal fossa, mylohyoid space, bronchial tree and lungs, and esophagus and gastrointestinal tract. Dr Hossaini noted that this may arise due to poor diagnostic imaging, a lack of anatomic recognition, inadequate visualization, improper dissection and retraction, excessive elevation or force, or poor elevation technique. Affected patients require close observation, and may need oral antibiotic therapy. If surgical removal of the displaced tooth or implant is required, intraoperative radiography and fluoroscopy may be necessary. This is also a preventable problem, and action must be taken to prevent its recurrence, including making improvements in patient preoperative evaluation as well as case–selection criteria.
Nerve damage: Nerve damage is another common complication in outpatient dental practice, most commonly in association with implant placement. Other associations include tooth extraction, endodontic treatment, LA injection, trauma, infection, and the presence of pathologic lesions in the oral cavity. Nerve damage typically arises from improper or inadequate preoperative or postoperative patient evaluation, treatment implementation, management of complications, or referral.
Preoperative or postoperative patient evaluation: Dr Hossaini highlighted the need to ensure preoperatively that a particular procedure is actually indicated, and to consider alternative techniques if appropriate. Diagnostic imaging should also be considered, as necessary. Although intraoral radiography has minimal or no surgical diagnostic value, extraoral imaging techniques such as panoramic radiography or cone beam computed tomography may be valuable in some cases. The patient's medical history should also be thoroughly reviewed.
Dr Hossaini noted that implant–related nerve injury can be indirect or direct.
Indirect: This arises in association with retraction or displacement of graft material, as well as edema, hematoma formation, and infection. Common causes include poor flap design and retraction, poor flap hygiene, a lack of anatomic recognition, inadequate hemostasis prior to closure and patient discharge, and inadequate understanding of the patient's medical history.
Direct: This typically arises in association with osteotomy, compression, or implant displacement. It is commonly caused by inadequate risk stratification in particular, as well as poor treatment planning, anatomic recognition, or surgical technique.
Affected patients require careful observation for at least 2 to 4 weeks initially. Observation is typically indicated in cases where there is no evidence of nerve transection, where the altered sensation is consistent with paresthesia, or where the patient is improving rapidly. However, some may require referral to a dental specialist with expertise in dealing with nerve injury, particularly in cases involving nerve transection or no signs of improvement, or where it is difficult to evaluate nerve function and pathology, or the patient is experiencing dysesthesia, or anesthesia without signs of improvement.
IMPLANT–RELATED COMPLICATIONS
According to Dr Hossaini, common implant–related complications include nerve damage, implant displacement, implant failure or ailing, and graft complications. He added that additional factors such as infection and bone or soft tissue loss may also compromise treatment and contribute to failure.
In his concluding remarks, Dr Hossaini also emphasized the need to be aware of medical complications in patients, particularly medical conditions that mimic dental conditions, and medication–related osteonecrosis associated with treatment with antiresorptive or anti–angiogenic agents.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.