

Summary
Although the 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care recommend stopping compressions during defibrillation, there is no convincing evidence in the literature to support this practice. This article reviews data confirming the importance of minimizing compression pauses during defibrillation of patients in cardiac arrest.
- Critical Care
- Myocardial Infarction
- First Aid
- Emergency Medicine
- Critical Care
- Myocardial Infarction
- First Aid
J. Scott Wieters, MD, Texas A&M University, Temple, Texas, USA, reviewed data confirming the importance of minimizing compression pauses during defibrillation of patients in cardiac arrest.
Although the 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care recommend stopping compressions during defibrillation, Dr Wieters stated that there is no convincing evidence in the literature to support this practice. From 1986 to 1990, 13 injuries were reported with “hands-on” defibrillation, most consisting of mild shocks or burns. In experimental models of hands-on defibrillation, current leakage (mean, 283 ± 140 μA; range, 18.9 to 907 μA) was within the acceptable safety limits [Lloyd MS et al. Circulation. 2008].
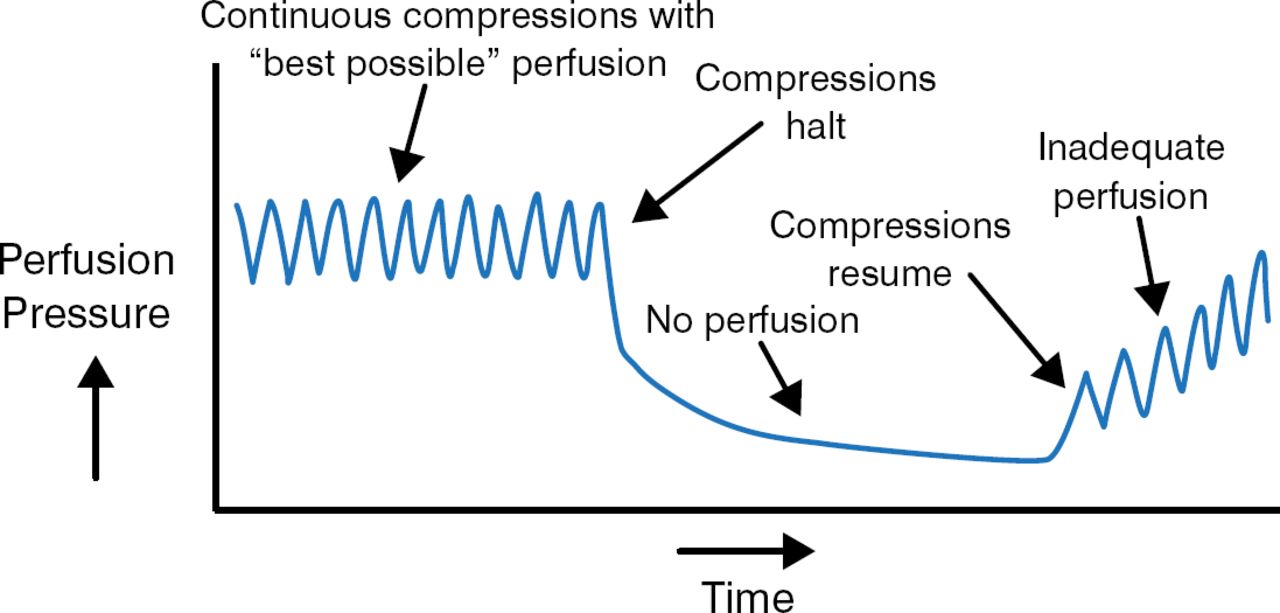
At the same time, there is substantial evidence indicating that interruptions in chest compression pauses should be avoided at all costs. Cardiac perfusion drops off dramatically when chest compressions stop, and perfusion takes time to rise when compressions resume (Figure 1). In one study, if the preshock pause was > 10 seconds, return of spontaneous circulation (ROSC) decreased by 50% [Eftestøl T et al. Circulation. 2002].

Effect of Compression Pauses on Cardiac Perfusion
Adapted from American Journal of Emergency Medicine, 30, Cunningham LM et al, Cardiopulmonary resuscitation for cardiac arrest: the importance of uninterrupted chest compressions in cardiac arrest resuscitation, 1630–1638. Copyright (2012), with permission from Elsevier.
In another study, when preshock pauses were < 3 seconds, the ROSC was 6 times higher. Keeping postshock pauses to < 6 seconds led to 18 times more ROSC [Edelson DP et al. Resuscitation. 2006]. In a large multicenter trial of 815 patients with out-of-hospital (OOH) cardiac arrest, patients with a preshock pause of < 10 seconds had 50% less mortality when compared with patients with a preshock pause > 20 seconds [Cheskes S et al. Circulation. 2011]. Every 5-second delay led to 18% mortality.
Dr Wieters emphasized that compressions should certainly continue during preshock charging and that, after defibrillation, end tidal carbon dioxide should be employed in place of pulse checks to monitor perfusion.
In a prospective observational cohort study of 506 cases of OOH cardiac arrest, the best survival (28.7%) was seen when the compressions were performed 60% to 80% of the total resuscitation time [Christensen J et al. Circulation. 2009]. Physicians should therefore aim for a chest compression fraction > 80%. Dr Wieters concluded by stating that a shock delivered with perfusion pressure at its peak will more likely result in ROSC.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.