

Summary
The Supplemental Nutrition Assistance Program (SNAP) provides federal funds to low-income persons to purchase food to address food insecurity and improve nutrition and health. SNAP has had a substantial antipoverty impact, improved metabolic outcomes, and improved dietary intake and health status, as discussed in this article.
- Obesity
- Prevention & Screening
- Pediatric Nutrition
- Nursing
- Nutrition Physiology
- Endocrinology
- Diabetes & Metabolic Syndrome
- Obesity
- Prevention & Screening
- Pediatric Nutrition
- Nursing
- Nutrition Physiology
The Supplemental Nutrition Assistance Program (SNAP) provides federal funds to low-income persons to purchase food to address food insecurity and improve nutrition and health. About 1 in 7 Americans receive SNAP benefits, with a higher rate in poorer states, and the average monthly household benefit is $275 [US Dept of Agriculture (USDA), Food and Nutrition Service (FNS). Characteristics of Supplemental Nutrition Assistance Program Households: Fiscal Year 2012. Report No. SNAP-14-CHAR. Alexandria, VA, 2014; USDA, FNS. Building a Healthy America: A Profile of the Supplemental Nutrition Assistance Program. Alexandria, VA, 2012]. SNAP has had a substantial antipoverty impact, lifting 5 million Americans higher than the poverty line, including 2 million children, stated James D. Weill, Food Research and Action Center, Washington, DC, USA. In addition to improving food security, SNAP has improved dietary intake and health status, especially among children, and improved metabolic outcomes, he stated. SNAP also has an economic impact in each community, because the funds are spent in the local markets.
SNAP serves a diverse population, including seniors, persons with disabilities, working families, and the unemployed. About 75% of SNAP households include children, and about 20% a senior or person with disability [USDA, FNS. Characteristics of Supplemental Nutrition Assistance Program Households: Fiscal Year 2012. Report No. SNAP-14-CHAR. Alexandria, VA, 2014]. Of the households receiving SNAP funds, 83% have a gross income lower than 100% of the federal poverty line, and about 60% are lower than 75% of the federal poverty line.
Despite the benefits and strengths of SNAP, improvements are needed to improve the nutrition and health of Americans in terms of sufficient food and its quality. Lisa Harnack, DrPH, RD, University of Minnesota, Minneapolis, Minnesota, USA, noted that the diet consumed by participants of SNAP is less consistent with dietary guidelines compared with the diets of other low-income and higher-income Americans, based on a number of surveys and cross-sectional analyses. Weill stated that a recent research summary from the USDA found that participants in SNAP value nutrition as much as nonparticipants, but that time and money constraints complicate the task of making healthy food choices [Mancino L, Guthrie J. Amber Waves. 2014. http://www.ers.usda.gov/amber-waves#.VGtOWGe-3-0. Accessed Nov 18, 2014].
Weill stated that strategies to improve SNAP include:
-
Ensuring all eligible persons receive SNAP benefits (1 in 5 do not)
-
Ensuring a full entitled benefit per participant
-
Increasing the monthly benefit
-
Increasing the availability of stores with SNAP-eligible foods
-
Providing nutrition education
-
Conducting research to identify successful nutrition education programs
The gains made by increasing the monthly benefit were shown by a natural demonstration project, that is, the increased SNAP benefit of 13.6% from 2009 to 2013 as a result of the American Recovery and Reinvestment Act [USDA, Economic Research Service. Food Security Improved Following the 2009 ARRA Increase in SNAP Benefits, Economic Research Report No. 116. Washington, DC, 2011]. Food insecurity and very low food insecurity were each reduced by 2 percentage points, participants ran out of funds later in the month, the number of monthly food transactions increased, and parents reported the health of their young children was better, stated Weill. More research is needed to fully understand the impact of the increased monthly benefit.
Increasing the consumption of fruits and vegetables is a goal to increase the nutrition and health of participants of SNAP. Among the programs evaluating such strategies is the Healthy Incentives Pilot (HIP) by the USDA and the Grocery Assistance Program Study (GAPS) by the University of Minnesota.
HIP tested whether financial incentives at the point of sale increased the consumption of targeted fruit and vegetables (TFV) [USDA, FNS. Evaluation of the Healthy Incentives Pilot (HIP): Final Report. Alexandria, VA, 2014]. Participants received a 30% incentive as a credit to their SNAP account for the purchase of TFV, defined as fresh, frozen, canned, or dried fruits and vegetables without added sugar, salt, or oils. Juice, white potatoes, and mature legumes were excluded. HIP randomized 9286 adults to the HIP group and 59 652 adults to the non-HIP group, and interviews were conducted with a subset from each group at 3 different times during the study that was conducted between July 2001 and December 2012.
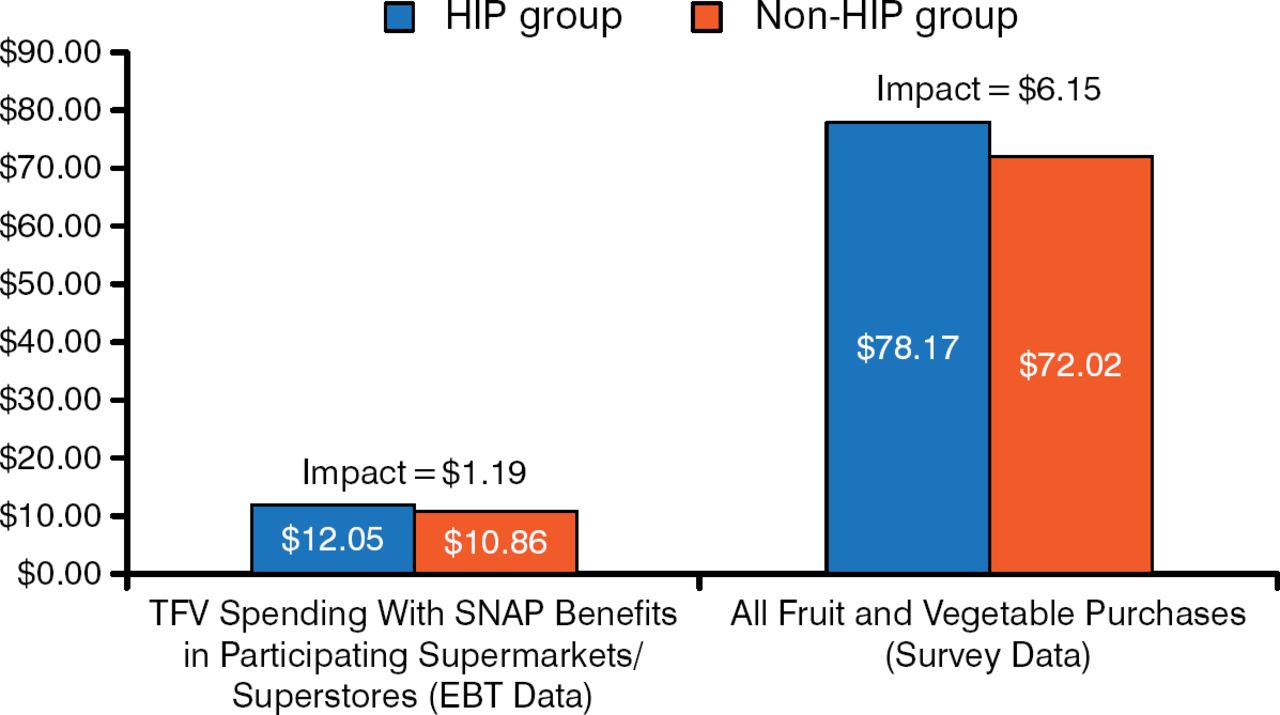
The HIP group, compared with the non-HIP group, consumed 0.24 more cup-equivalents per day of TFV (P < .01). This modest effect was a substantial relative increase when considered in relation to the low TFV intake by Americans and participants of SNAP in general, stated Parke Wilde, PhD, Tufts University, Medford, Massachusetts, USA. Based on purchases of TFV at SNAP-participating centers, the average incentive was $3.65, which was lower than anticipated. However, participants in the HIP group reported an overall increase in FV purchases (Figure 1); thus, it is believed that purchases were also made at SNAP nonparticipating centers. Regardless of the proximity of supermarkets, where 78.6% of the SNAP funds in HIP were spent, the purchase of TFV increased by about $11 to $13.

Monthly Purchases of Fruit and Vegetables by HIP Participants
EBT, electronic benefit transfer; HIP, Healthy Incentives Pilot; SNAP, Supplemental Nutrition Assistance Program; TFV, targeted fruits and vegetables.
United States Department of Agriculture. Food and Nutrition Service. Healthy Incentives Pilot Final Evaluation Report. Exhibit. ES.2, page 5. September 18, 2014. http://www.fns.usda.gov/healthy-incentives-pilot-final-evaluation-report. Accessed November 26, 2014.
The ongoing GAPS is evaluating the independent and combined effects on dietary intake of prohibiting the purchase of foods high in discretionary calories (sugar-sweetened beverages, sweet baked goods, and candy) with SNAP benefits and incentivizing (30% credit) the purchase of FV.
A total of 320 low-income adults who are not SNAP participants will be randomized in 3 different waves after a 1-month baseline period to 1 of 4 study arms: control (usual SNAP usage), restricted benefit, FV incentive, and restricted benefit plus FV incentive. The follow-up is 3 months.
Of the 135 participants to date, 80.3% are women, 53% are African American, and 9% are Hispanic or Latino. The proportions who are overweight or obese is 26% and 55%, respectively. The proportion with low and very low food security is 33% and 48%; past participation in SNAP is 52%, and it is 12% for the Women, Infants, and Children nutrition program (current participation is 10%). Emergency food assistance was used by 54% in the previous 12 months. Adherence to the experimental procedures is fair, with the mean number of infractions reduced from 1.18 for month 1 to 0.87 for month 3.
The feasibility of the GAPS methodology of a mock food-assistance program to study proposed modifications to SNAP has been demonstrated, said Dr Harnack. However, some methodology issues may be the external validity of the study, because the sample may not be representative of households that participate in SNAP. Also, only 1 benefit level is being studied, but SNAP has lower and higher levels. The short duration of exposure (3 months) is limited, and long-term results may differ.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.