

Summary
Weight stigma is defined as negative attitudes toward persons because of their excess body weight, including such stereotypes as their being at fault for their weight and their lacking willpower and discipline. Substantial evidence also exists of weight bias and prejudice in the media, employment, education, and health care. This article discusses that impact on patient behavior and health, as well as strategies to eliminate discrimination.
- Obesity
- Nursing
- Obesity
- Nursing
- Endocrinology
- Diabetes & Metabolic Syndrome
- Exclusive Article - For home page
Weight stigma is defined as negative attitudes toward persons because of their excess body weight, including such stereotypes as their being at fault for their weight and their lacking willpower and discipline. These stereotypes are rarely challenged and then become socially acceptable, leading to bullying, prejudice, and discrimination. Notably, weight stigma is diverse, affecting men and women, all age groups, groups of both low and high income and education, all races and ethnic groups, and all body weight strata [Andreyeva T et al. Obesity (Silver Spring). 2008]. Substantial evidence also exists of weight bias (WB) and prejudice in the media, employment, education, and health care, stated Rebecca M. Puhl, PhD, Yale University, New Haven, Connecticut, USA.
Health care professionals (HCPs), including physicians, are not immune to WB and negative stereotypes. In a study investigating potential sources of WB, 2449 women (mean body mass index [BMI], 37.6 kg/m2; mean age, 49.9 years) reported WB from physicians (69%), nurses (46%), dietitians or nutritionists (37%), and mental health professionals (21%) [Puhl RM, Brownell KD. Obesity (Silver Spring). 2006]. Research confirms WB's impact on HCPs' interactions with patients, which then can negatively affect patients' behaviors, including lower trust in their primary care physicians, avoidance of health care, and obesity-promoting responses such as binge eating.
In a survey of 4732 first-year medical students, 67% and 74% expressed explicit and implicit WB, respectively [Phelan SM et al. Obesity (Silver Spring). 2014]. This WB was especially prevalent in students who were men, white, or Hispanic and who had lower BMI, mirroring the general public, said Dr Puhl. WB was found among clinical-level medical students in their interactions with virtual patients with or without obesity and standardized behaviors—including stereotyping, less physical contact, and more assigning of responsibility for weight-related complaints [Persky S, Eccleston CP. Int J Obes (Lond). 2011]. Yet, another study found that 97% of 107 HCP trainees stated that fat jokes were not acceptable, but they had witnessed such jokes and derogatory comments by instructors (40%) and practicing HCPs (65%) [Puhl RM et al. Obesity (Silver Spring). 2013]. Furthermore, although 80% of HCP trainees stated that they were confident about treating obesity, 36% said that they felt frustrated caring for patients with obesity; 33% thought that their patients lacked motivation; and 36% thought that their patients were noncompliant with treatment.
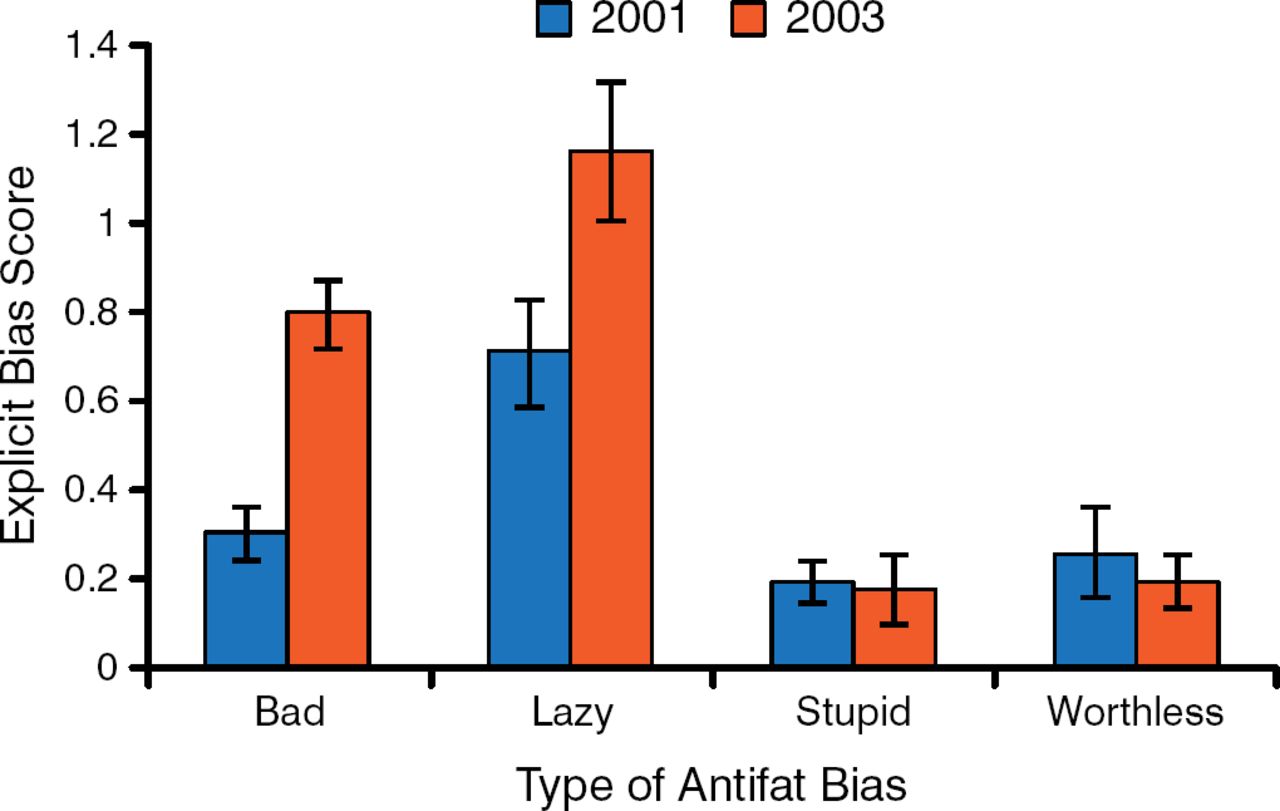
WB is expressed even among obesity researchers and HCPs, with an increase in explicit bias scores in a survey of attendees of ObesityWeek 2013 when compared with the 2001 survey of the same population (Figure 1) [Tomiyama AJ et al. Obesity (Silver Spring). 2014].

Rates of Explicit Bias in a Survey of ObesityWeek 2013 Attendees
Adapted from Tomiyama AJ et al. Weight bias in 2001 vs 2013: contradictory attitudes among obesity researchers and health professionals. Obesity. Published online Early View Oct 8 2014. DOI 10.1002/oby.20910. With permission from the Obesity Society.
IMPACT ON PATIENT BEHAVIOR AND HEALTH
Dr Puhl stated that, in the last decade, it has become more common for patients to avoid health care because of WB. As reported in one study of nearly 500 women, patients had high access to care for gynecologic screenings and mammograms yet delayed preventive services because of disrespect and negative attitudes from HCPs, embarrassment of being weighed, and medical equipment being too small; as BMI increased, so did the barriers to health care [Amy NK et al. Int J Obes (Lond). 2006]. Adult patients with obesity reported switching their primary care physicians because they believed that they were treated negatively because of their weight [Gudzune KA et al. Obesity (Sliver Spring). 2014].
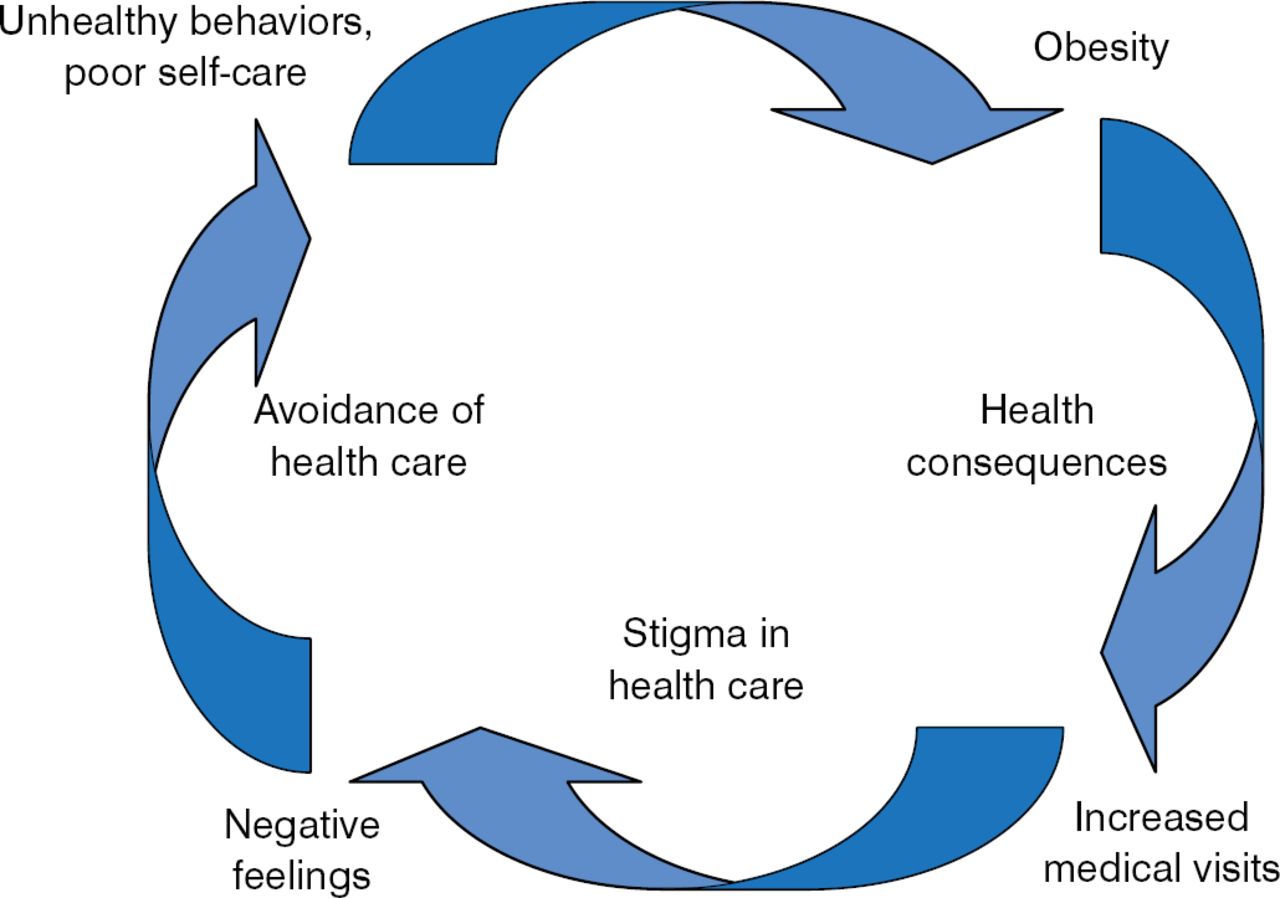
The cycle of stigma and obesity (Figure 2) is fed by WB and the lack of trust in HCPs. Individuals who experience WB are at increased risk for health consequences, including poor eating behaviors, decreased physical activity, weight gain and obesity, psychological distress, and physiologic responses. Binge eating as a result of internalizing WB has been found in adults [Durso LE et al. Obes Facts. 2012; Friedman KE et al. Obesity (Silver Spring). 2008] and youth [Quick V et al. Int J Behav Nutr Phys Act. 2013; Puhl RM, Luedicke J. J Youth Adolesc. 2012]. Other studies have shown an association between internalization of WB and health-related quality of life [Latner JD et al. Eat Behav. 2014; Lillis J et al. J Health Psychol. 2011], impairment of physical and mental health [Latner JD et al. J Eat Disord. 2013], and lower global health [Hilbert A et al. Obesity (Silver Spring). 2014].

The Cycle of Stigma and Obesity
Reproduced with permission from RM Puhl, PhD.
Increased physiologic stress has been identified in persons who perceive experiencing weight discrimination, as estimated by increased levels of C-reactive protein, blood pressure, cortisol, HbA1c, and oxidative stress [Schvey NA et al. Psychom Med. 2014; Sutin AR et al. Obesity (Silver Spring). 2014; Tomiyama AJ et al. Health Psychol. 2014; Tsenkova VK et al. Ann Behav Med. 2011].
Notably, weight stigma may pose barriers to weight loss in persons who undertake weight-loss treatment, and it is associated with increased calorie intake, decreased energy expenditure, and lower likelihood of achieving clinically significant weight loss in such patients [Gudzune KA et al. Prev Med. 2014; Carels RA et al. Eat Weight Disord. 2009]. Persons seeking weight-loss surgery reported WB, regardless of their BMI, sex, or age. One study reported symptoms of depression and significantly less weight loss 1 year after weight-loss surgery in adults who had higher levels of WB internalization [Lent MR et al. Obes Surg. 2014].
STRATEGIES TO ELIMINATE WB AND DISCRIMINATION BY HCPS
Professional medical societies are starting to address WB among HCPs. Documents to highlight this issue and assist HCPs have been published, including position papers from the Institute of Medicine and the Obesity Society and resources from the American Medical Association website. Dr Puhl stated that efforts to address obesity by HCP must include:
-
Increased attention to WB and its consequences
-
Use of “people-first,” respectful language with patients, colleagues, and students
-
Avoidance of strategies that shame and blame
-
Removal of stigma from existing efforts
-
Support and empowerment rather than shame or stigmatization
-
Adjustment of the office environment for patients with overweight and obesity (size of equipment, space, and furniture)
The use of people-first language is respectful and can help reduce stigma and discrimination by describing a person as having a disease or condition, rather than by identifying the person as a disease or condition. This involves referring to a person with overweight or obesity, not as an overweight or obese person. Studies have identified terminology that is acceptable or preferred by persons with overweight or obesity, such as high BMI, excess weight, and unhealthy weight [Puhl R et al. Int J Obes (London). 2013; Puhl RM et al. Pediatrics. 2011].
Education of medical students and trainees in health professions through education videos and lectures about WB and obesity has shown promise in increasing empathy, confidence in interacting with patients with higher weight, and understanding the role of genetics and environment in obesity and in decreasing negative stereotyping and WB [Kushner RF et al. BMC Med Educ. 2014].
Dr Puhl stated that stigma is known to undermine health and that public health policies and programs have addressed stigma in relation to cholera, leprosy, drug addiction, and HIV/AIDS, among others. However, obesity remains a glaring omission from this list.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.