

Summary
Three new obesity guidelines have been developed that should improve the management of this condition and its associated comorbidities. This discussion includes the development of recommendations on best practices in obesity treatment, overview of the American Association of Clinical Endocrinologist Obesity Guidelines, as well as a review of the American Society of Bariatric Physicians guidelines.
- Nutrition Guidelines
- Obesity
- Diabetes & Endocrinology Guidelines
- Obesity
- Nutrition Guidelines
- Endocrinology
- Diabetes & Metabolic Syndrome
- Diabetes & Endocrinology Guidelines
Three new obesity guidelines have been developed that should improve the management of this condition and its associated comorbidities. Michael D. Jensen, MD, Mayo Clinic College of Medicine, Rochester, Minnesota, USA, discussed the development of recommendations on best practices in obesity treatment, and he described the development of the American Heart Association/American College of Cardiology/The Obesity Society (AHA/ACC/TOS) Obesity Guidelines [Jensen MD et al. J Am Coll Cardiol. 2014]. In developing these guidelines, the ACC, AHA, and partner organizations collaborated with the National Heart, Lung, and Blood Institute (NHLBI) in an evidence-based approach, using systematic reviews of the literature and graded recommendations. The NHLBI systematic review and guideline development process included identifying topic areas; developing critical questions; searching for all eligible studies; evaluating, summarizing, and grading the evidence; developing recommendations; and developing, reviewing, revising, and disseminating the guidelines.
The highest-rated evidence included that derived from well-designed, randomized clinical trials (RCTs) or meta-analyses of such trials. Initially, more than 20 critical questions (CQs) were identified, of which 5 were chosen based on perceived importance and resources (Table 1).
Critical Questions Addressed in the AHA/ACC/TOS Obesity Guidelines
The recommendations of the obesity panel of experts that crafted the guidelines are summarized in Table 2. Identification of patients who need to lose weight is based on meta-analyses and systematic reviews because of the great volume of data; others are based on RCTs.
Summary of Recommendations for Obesity
There are gaps in the AHA/ACC/TOS Obesity Guidelines, including pharmacotherapy. In addition, there are also no critical questions on physical activity protocols or weight gain caused by medications.
Another guideline was developed by the American Association of Clinical Endocrinologists (AACE), which used a different approach. An overview of the AACE Obesity Guidelines [Mechanick JI. Endocrine Practice. 2014] was presented by Jeffrey Mechanick, MD, Icahn School of Medicine at Mount Sinai, New York, New York, USA.
The AACE Obesity Guidelines are an algorithm that is part of a larger comprehensive algorithm designed to optimize the care of patients with diabetes. This algorithm stresses prevention over treatment-oriented disease management. For diabetes, it moves from HbA1c-centric care to comprehensive care; for obesity, it is moving from defining obesity using weight and body mass index (BMI) to care that is complication-centric. The AACE guidelines include a level of subjectivity and, unlike the AHA/ACC/ TOS Obesity Guidelines, are not purely evidence based [Garber AJ et al. Endocrine Practice. 2013].
BMI is included in the algorithm because it is used to determine prescribing indications for pharmacotherapy. Cardiometabolic disease risk can be assessed using standard scoring systems. Therapies are suggested based on the risk for complications. There are currently not enough data to recommend a particular drug or bariatric procedure. Algorithms for other aspects of diabetic care, and a list of medications associated with weight loss or gain, are also available.
Dr Mechanick said that the strengths of the AACE algorithm are that it is based on the weight of evidence, does not rely solely on RCTs, and is part of a comprehensive strategy. It is a complication-centric, risk stratification preventive paradigm that recognizes roles for lifestyle, medicines, and surgery. Weaknesses, however, include a lack of defined lifestyle modifications, the continued incorporation of BMI cutoffs, and a lack of defined pharmacotherapy and surgical options.
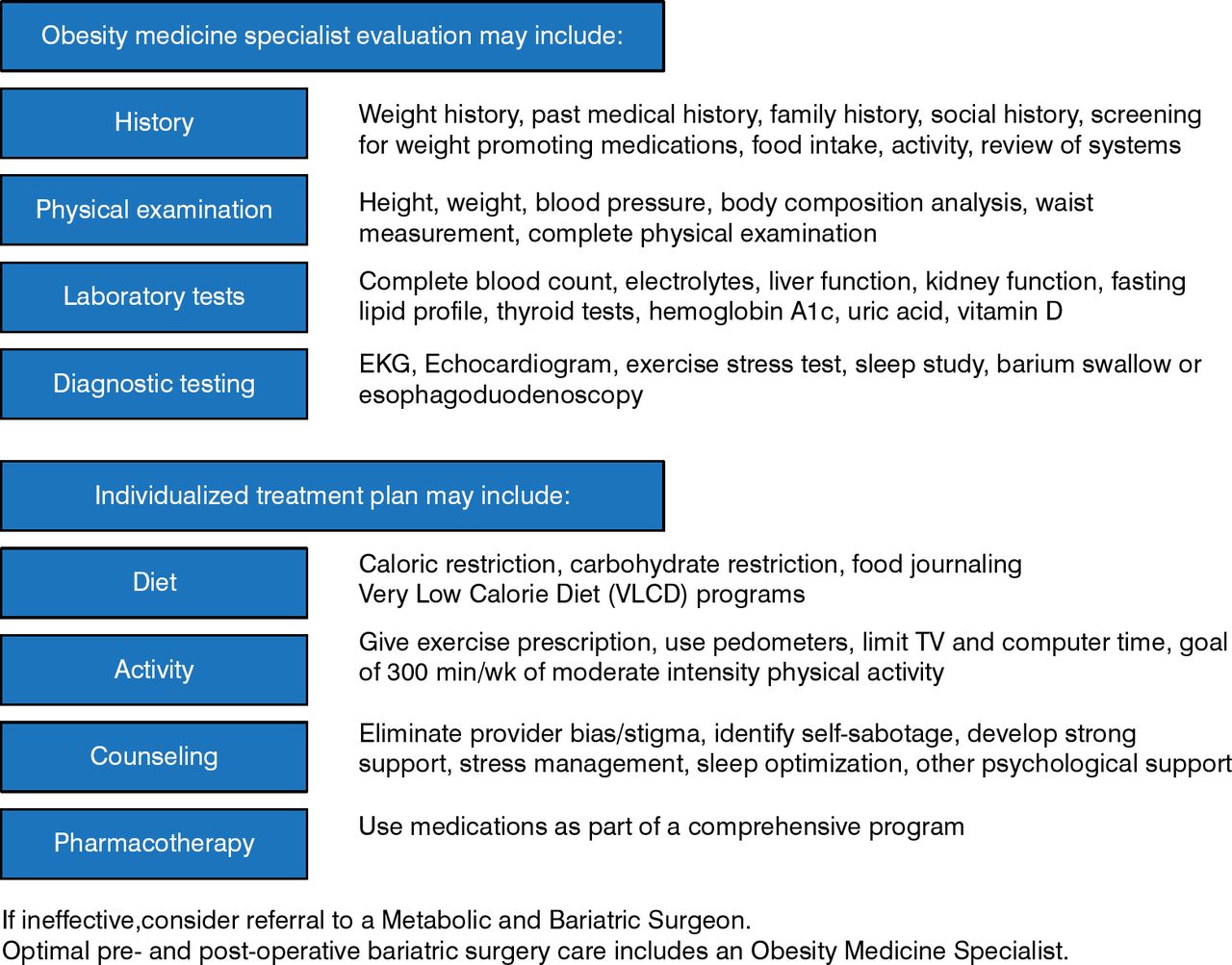
The American Society of Bariatric Physicians (ASBP) has also developed an obesity guideline and algorithm (Figure 1) [Seger JC et al. ASBP Obesity Algorithm. 2013], which was discussed by Wendy M. Scinta, MD, American Society of Bariatric Physicians, Aurora, Colorado, USA. Dr Scinta pointed out that all obesity guidelines are complementary, not competitive. The ASBP algorithm is based on scientific evidence, supported by the medical literature, and derived from the clinical experiences of members of the ASBP.

ASBP Obesity Algorithm Executive Summary
Seger JC, Horn DB, Westman EC, Lindquist R, Scinta W, Richardson LA, Primack C, Bryman DA, McCarthy W, Hendricks E, Sabowitz BN, Schmidt SL, Bays HE. Obesity Algorithm®, presented by the American Society of Bariatric Physicians®. www.obesityalgorithm.org (accessed December 2, 2014). ©American Society of Bariatric Physicians® 2013–2014: used with permission.
The algorithm includes overall management goals, examinations and tests, and treatment modalities. Two components of obesity as a disease include adiposopathy (sick fat disease), a derangement of fat cells that causes complications of the endocrine and immune systems (eg, elevated blood lipids and glucose); and fat mass disease, associated with stress on tissues (eg, leading to joint damage and sleep apnea).
Practitioners should focus on the individual because patients have different backgrounds that contribute to their obesity. Therefore, a thorough history should be taken, followed by a comprehensive physical examination and general and obesity-relevant laboratory tests, some of which will be patient specific, such as an echo-cardiogram if it shows abnormalities. Other tests could include resting metabolic rate and body com position analysis, which can be measured in a variety of ways.
Obesity treatment medicine should include nutrition, behavioral modification, physical activity, and medical management. Secondary and contributing causes like sleep apnea, bulimia, rare genetic disorders, or insulinoma should be ruled out or treated. Medications that are used to treat obesity-related comorbidities or other conditions can cause obesity (eg, some antidiabetic drugs and antiseizure medications). Another drug that does not cause weight gain can be identified and substituted.
Both Dr Jensen and Dr Scinta emphasized that the diet that works is the one the patient will follow. Among the useful options are negative caloric balance diets, meal substitutes, and low-carbohydrate diets. Also of importance is having the patient develop a maintenance plan. Physical activity is more important for maintenance than weight loss but has advantages even in the absence of weight loss, and ideally it should include aerobic and strength training.
Another important aspect of the ASBP algorithm is the use of motivational interviewing; although there is not a lot of evidence behind it, listening while the patient figures out issues rather than jumping in and giving advice may be helpful. Other behavioral components include stimulus control by restructuring the home environment, and cognitive restructuring, such as keeping a food and mood diary.
Only 3 weight management pharmacotherapies are currently approved: lorcaserin, phentermine HCl/ topiramate extended-release, and naltrexone/bupropion extended release. Additional agents are expected to be approved soon.
High-quality treatments for obesity are available and can produce medically important weight loss; these must be tailored to the individual patient to improve the chances for success.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.