

Summary
The effect of diabetes on muscles, tendons, bones, and ligaments often goes unrecognized. This article describes a number of musculoskeletal complications and how they affect patient care and outcome in people with diabetes. These musculoskeletal complications, which can become painful and cause patients to alter their daily routines, have a higher prevalence among those with long-standing type 1 and type 2 diabetes.
- Bone Density & Structure Disorders Diabetes & Metabolic Syndrome
- Orthopaedic Pain Management
- Diabetes Mellitus
- Orthopaedics & Sports Medicine
- Endocrinology
- Diabetes & Metabolism
The effect of diabetes on muscles, tendons, bones, and ligaments often goes unrecognized. Fred Wendler, DPT, Bloomington, Illinois, USA, described a number of musculoskeletal complications and how they affect patient care and outcome in people with diabetes. These musculoskeletal complications, which can become painful and cause patients to alter their daily routines, have a higher prevalence among those with long-standing type 1 and type 2 diabetes (Table 1). A variety of mechanisms for these musculoskeletal complications has been described, including microvascular abnormalities, excess collagen accumulation, or metabolic perturbations.
Prevalence of Musculoskeletal Disorders in People With and Without Diabetes (in Percentages)
Diabetes can also affect the shoulder, causing reflex sympathetic dystrophy (RSD) and adhesive capsulitis. RSD, or complex regional pain syndrome, is a chronic pain syndrome that can also affect the arms, hands, legs, and feet. Symptoms include pain, swelling and edema, skin color changes, abnormal sweating, and changes in the nails. RSD spreads through the whole limb and other parts of the body, and it often gets worse before it gets better. There are 2 types of RSD. RSD 1 is a chronic nerve disorder that occurs after a musculoskeletal injury. RSD 2, also called causalgia, is caused by a specific injury to a nerve. These conditions are both treated with physical therapy, medications, nerve blocks, spinal cord stimulation, and psychological counseling.
Adhesive capsulitis, or frozen shoulder, is a painful progressive condition that restricts shoulder motion and may be bilateral or unilateral. Treatment options include physical therapy, corticosteroid injections, manipulation, and even surgery.
Carpal tunnel syndrome (CTS), cheiroarthropathy, Dupuytren contracture, and flexor tenosynovitis are musculoskeletal complications of the wrist and hand. CTS is characterized by inflammation and swelling due to overuse, injury, or health-related problems. CTS occurs when there is thickening of the tissues and transverse carpal ligament that results in a narrowing of the space in the carpal tunnel. Compression of the median nerve leads to pain, paresthesia, and sensory loss in the areas served by it. CTS occurs in 20% to 25% of people with diabetes, and the duration of diabetes increases the risk of developing it [Crispin JC, Alcocer-Varela J. Am J Med 2003; Kim RP et al. Clin Diabetes 2001]. Treatment of CTS consists of oral anti-inflammatory medications, local injection of corticosteroids, or surgical procedures to release pressure on the median nerve.
Diabetic cheiroarthropathy (DC)—also called diabetic stiff hand syndrome or limited joint mobility syndrome—is characterized by thick, tight, waxy skin, leading to decreased range of motion in both flexion and extension. DC can affect the metacarpophalangeal and proximal interphalangeal joints and, eventually, the distal interphalangeal joints. Therapy consists of optimizing glycemic control and utilizing physical therapy to maintain range of motion.
Dupuytren contracture, also called Dupuytren disease, occurs in 16% to 42% of people with diabetes [Kim RP et al. Clin Diabetes 2001], and it is thought to be related to collagen changes, diabetic microangiopathy, and diabetic neuropathy. It is characterized by a thickening and shortening of the palmar fascia, and it occurs in 3 stages. Stage 3, the most advanced, presents as a flexion contraction, usually of the fourth finger. It is treated with oral anti-inflammatory medications, splints, hand therapy, and sometimes local injections of corticosteroids. In severe cases, surgical procedures designed to reverse the contractures and restore normal hand functions may be necessary.
Flexor tenosynovitis, or trigger finger, is a condition in which a nodule or thickening will develop on the tendon of the affected finger. This can catch the tendon as it slides through the opening of the tunnel. Patients with type 1 diabetes are at particularly increased risk. Treatment strategies similar to those used for Dupuytren contractures have been used with success.
Diabetic amyotrophy, diabetic muscle infraction, and decreased muscle strength are other musculoskeletal conditions often associated with diabetes. Diabetic amyotrophy is characterized by painful muscle wasting and weakness of the proximal lower extremity muscles. The prevalence increases among those with type 2 diabetes and older persons with diabetes. The condition presents as wasting of the thighs, hips, or buttocks, with thigh muscle atrophy. Weight loss, elevated protein levels in cerebrospinal fluid, and loss of the patellar tendon reflex are also possible. Treatment consists of ensuring that blood glucose levels are in the reference range and that the patient is on oral medications for pain.
Diabetic muscle infarction (DMI) is increasing in prevalence among patients with a long history of poorly controlled diabetes. DMI affects patients with an average age of 40 to 43 years (range, 19 to 81 years). It is more common in those with type 1 diabetes than those with type 2 diabetes [Trujillo-Santos AJ. Diabetes Care 2003]. Multiple microvascular complications, such as neuropathy, nephropathy, and retinopathy, can occur. DMI usually presents with a spontaneous or sudden onset of pain, swelling, or mass in the affected muscles—most commonly, the quadriceps. The diagnosis is made through a combination of clinical presentation, laboratory tests, magnetic resonance images, and biopsies. Treatment usually consists of rest and analgesics. Immobilization, antiplatelet agents, steroids, and surgery are sometimes used. DMI tends to resolve over a period of weeks to months (average, 4 weeks).
Elderly patients with diabetes are at higher risk of developing physical disability. This may be due to an acceleration in the loss of skeletal muscle strength that occurs more often in elderly people with type 2 diabetes [Park SW et al. Diabetes Care 2007].
Charcot joint—also known as Charcot foot, neuropathic arthropathy, or diabetic osteoarthropathy—is rare and occurs in just .1% to .4% of people with type 1 and type 2 diabetes [Kim RP et al. Clin Diabetes 2001]. It generally presents as a single swollen deformed joint that may or may not be painful. Peripheral neuropathy and skin deformities (eg, erythema, skin atrophy, soft tissue ulcers) will be present. Diagnosis of Charcot joint is based on clinical and radiologic findings. The treatment involves improving glycemic control. Casting or bracing to immobilize and protect against weight bearing or surgery may be necessary in some cases.
Diffuse idiopathic skeletal hyperostosis (DISH), also called Forestier disease, is characterized by calcification along the sides of the vertebrae and at the insertion sites of the ligaments and tendons to the vertebrae. The etiology of DISH remains unknown, but persons with type 2 diabetes are 3 times more likely than people without diabetes to be diagnosed with this disorder. Symptoms of DISH include pain, stiffness, and loss of range of motion. Difficulty swallowing or hoarseness can occur if the cervical spine is involved. The diagnosis is made through a combination of clinical presentation, radiographs, or magnetic resonance imaging. Currently, there is no cure, and the treatment is supportive.
Osteoporosis—a condition defined by low bone mass, increased fragility, decreased bone quality, and increased fracture risk—is also more common among people with diabetes.
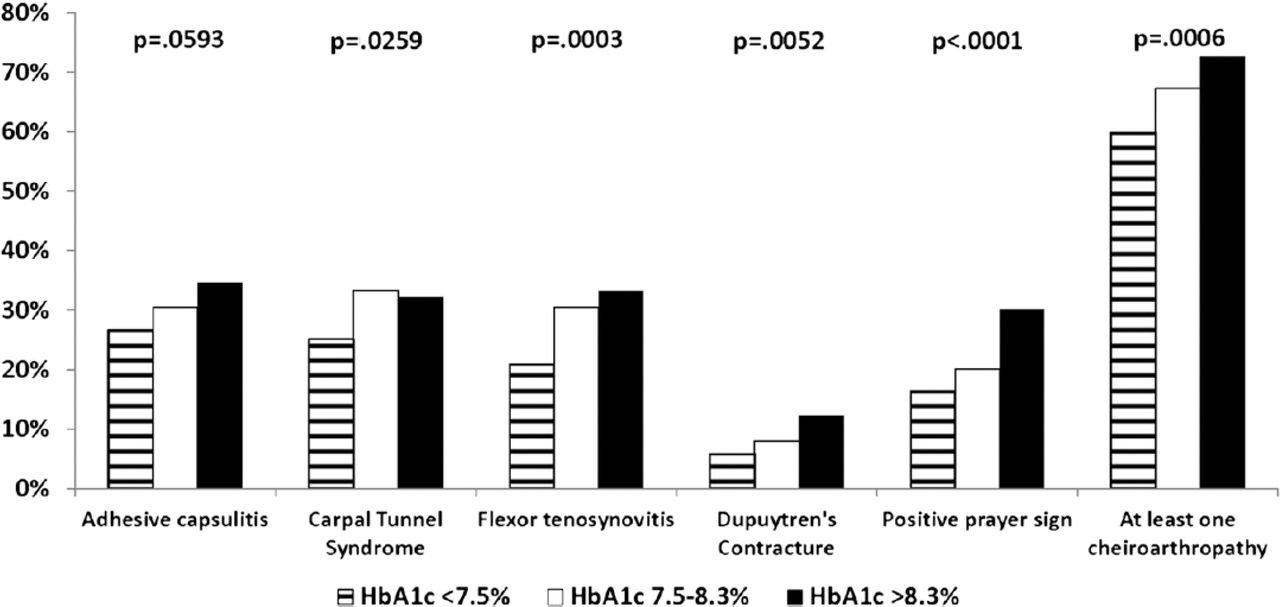
Maintaining blood glucose levels within the reference range is important to reducing most musculoskeletal complications of diabetes (Figure 1). Additionally, patients who seek early treatment and exercise have better outcomes.

Good Glucose Control Reduces Musculoskeletal Complications
Larkin ME et al. Musculoskeletal complications in type 1 diabetes. Diabetes Care. 2014;37:1863–1869. With permission from American Diabetes Association.
In closing, Dr. Wendler noted that patients with diabetes are at increased risk of many musculoskeletal disorders. Clinicians should work to recognize these complications to pursue interventions and treatments that will improve outcomes for this highrisk population.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.