

Summary
Surgical valve replacement or repair is the gold standard treatment of severe valvular heart disease and severe symptomatic valve stenosis [Guidoin R et al. Ann NY Acad Sci 2010]. This article discusses recent developments and challenges in the field of surgery for valvular disease.
- Interventional Techniques & Devices
- Valvular Disease
Surgical valve replacement or repair is the gold standard treatment of severe valvular heart disease and severe symptomatic valve stenosis [Guidoin R et al. Ann NY Acad Sci 2010]. Andrew Chukwuemeka, MD, FRCS, Imperial College Healthcare NHS Trust, London, United Kingdom (UK), discussed recent developments and challenges in the field of surgery for valvular disease.
In the past decade, there has been an exponential increase in percutaneous coronary intervention (PCI) compared with a leveling off of coronary artery bypass surgery in the UK (CABG; Figure 1). However, the decline in CABG has been offset by marked increases in the annual volume of aortic and mitral valve operations [The Society for Cardiothoracic Surgery in Great Britain & Ireland. Sixth National Adult Cardiac Surgical Database Report 2008].

Annual Incidence of PCI and CABG in the UK.
Reproduced with permission from A. Chukwuemeka, MD.
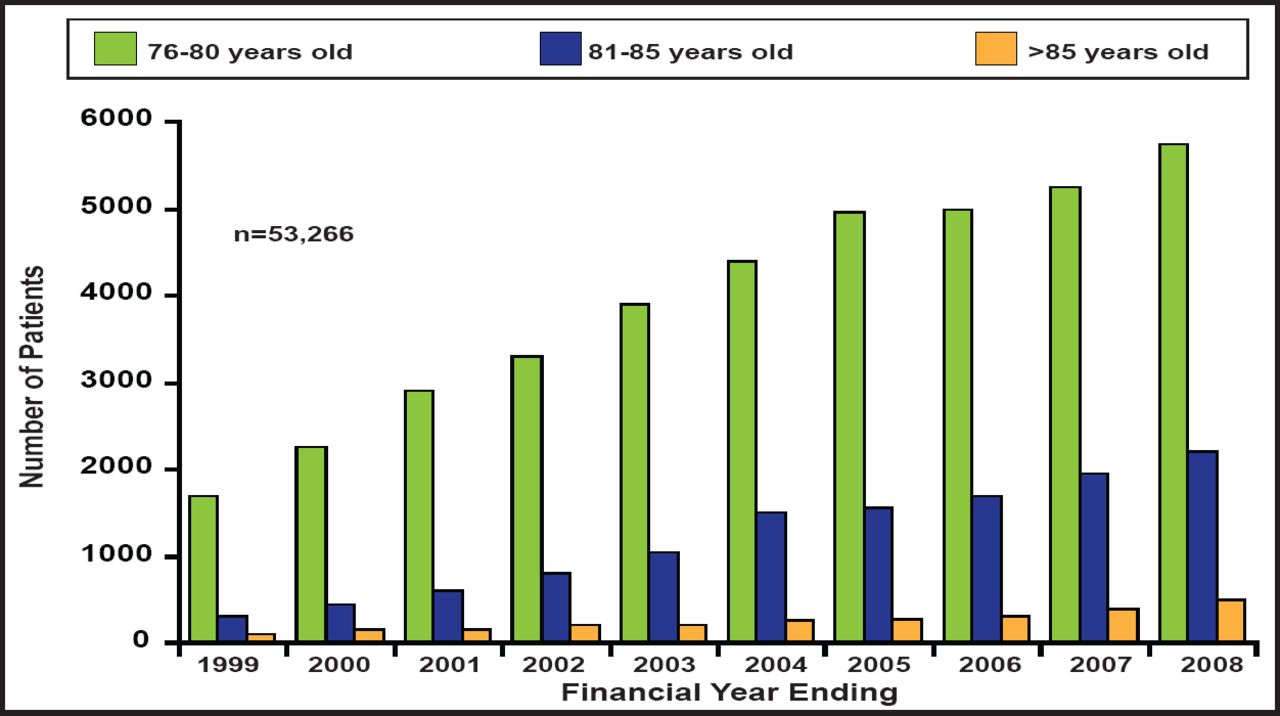
Many of these procedures were performed in elderly patients with multiple comorbidities—a challenging change in demographics for cardiac surgeons (Figure 2). In spite of increasing age, postoperative survival remains high. “The surgery is safe, effective, removes symptoms, extends survival, and improves quality of life,” said Prof. Chukwuemeka, noting that from 2004 to 2008, the survival rate in patients aged >80 years was 65% at 5 years after surgery, which is impressive, considering the patient population that is involved [The Society for Cardiothoracic Surgery in Great Britain & Ireland. Sixth National Adult Cardiac Surgical Database Report 2008].

Rise in the Number of Elderly Cardiac Surgery Patients.
Reproduced with permission from A. Chukwuemeka, MD.
The Challenges Ahead
Four main challenges lie ahead:
-
Adaptation to increasingly elderly patients with significant comorbidities
-
Reduction of prosthetic valve-related morbidity
-
Establishment of minimally invasive techniques
-
Improvement of risk assessment
As the population ages, the number of valve replacement surgeries is expected to increase sharply. Percutaneous aortic valve implantation provides an attractive alternative to standard open heart surgery in elderly patients who are considered to be at high or prohibitive surgical risk in large part due to their advanced age [Guidoin R et al. Ann NY Acad Sci 2010].
For patients aged >70 years with severe aortic stenosis, transcatheter aortic valve implantation (TAVI) may provide a promising alternative to surgical aortic valve replacement (AVR) [Guidoin R et al. Ann NY Acad Sci 2010; Leon MB et al. N Engl J Med 2010; Smith CR et al. N Engl J Med 2011]. For those with severe mitral regurgitation (MR), which also confers a poor prognosis (particularly in patients with heart failure) [Maisano F et al. Int J Cardiovasc Imaging 2011], catheter-based mitral repair systems offer a new option.
MitraClip, a percutaneous mitral valve (MV) repair device, has been compared with surgery in the Endovascular Valve Edge-to-Edge Repair Study (EVEREST II) randomized trial [Maisano F et al. Int J Cardiovasc Imaging 2011]. Two-year follow-up data from EVEREST II have shown that although a catheter-based MV repair procedure that uses the MitraClip system was less effective at reducing MR than conventional surgery, similar improvements in clinical outcomes were observed with fewer short-term adverse events [Cleland JG et al. Eur J Heart Fail 2011; Feldman T et al. N Engl J Med 2011].
Sutureless implantation of the prosthesis is another promising approach that has the potential to shorten aortic crossclamp time, thereby reducing morbidity and mortality in elderly and high-risk patients. A recent study found it possible to implant a well-functioning, sutureless, stent-mounted valve in the aortic position in less than 20 minutes of aortic crossclamping—a finding that was associated with excellent early clinical and hemodynamic outcomes in high-risk patients [Flameng W et al. J Thorac Cardiovasc Surg 2011].
Reducing Prosthetic Valve-Related Mortality
There is no perfect valve substitute. All prostheses, whether mechanical or biological, involve some compromise, and all introduce a new disease process: the prosthetic disease. Considerations for choosing between a mechanical valve and a bioprosthesis include hemodynamic performance, long-term durability, and the need for chronic anticoagulation [Goncalo F et al. Interact Cardiovasc Thorac Surg 2009].
There is a trend toward use of more bioprosthetic valves [Seeburger J et al. Cardiac Surgery 2009]. The main advantage with bioprosthetic valves is that they do not require lifelong anticoagulant therapy due to lower thrombotic risk, although mechanical valves are more durable. For most patients with a bioprosthetic valve, structural valve deterioration starts around 5 years postimplantation and increases rapidly [Tillquist MN, Maddox TM. Patient Prefer Adherence 2011].
Another option is reconstructive valve repair. For example, aortic valve-sparing operations in patients with Marfan syndrome provide excellent clinical outcomes: <1% operative mortality, 87.2% 15-year survival, and 79.2% freedom from more-than-mild aortic insufficiency at 15 years [David TE. J Thorac Cardiovasc Surg 2009].
Establishing Minimally Invasive Techniques
Controversy surrounds the use of minimally invasive AVR. A 2008 meta-analysis suggested marginal benefits in perioperative mortality (4667 patients; OR, 0.72; 95% CI, 0.51 to 1.00; p=0.05), intensive care unit stay, total hospital stay, and ventilation time in the minimal access AVR group. However, crossclamp, cardiopulmonary bypass, and total operation times were longer [Murtuza B et al. Ann Thorac Surg 2008]. Another meta-analysis showed that ministernotomy can be safely performed for AVR, without increased risk of death or other major complications; however, few objective advantages were observed [Brown ML et al. J Thorac Cardiovasc Surg 2009].
Improving Risk Assessment
In 1999, the EuroSCORE risk assessment system was recommended for widespread use [Nashef SA et al. Eur J Cardiothorac Surg 1999]. But, according to Prof. Chukwuemeka, its predictive assessment for individual patients was limited, and it was a poor tool for valvular heart disease compared with other cardiac surgeries (only 30% of patients in the dataset).
A recent report by The Working Group on Valvular Heart Disease of the European Society of Cardiology reviewed the most widely used risk scores (EuroScore, STS, and Ambler score) and concluded that current risk scores do not provide reliable estimates of exact operative mortality in individual valvular heart disease patients. Scores should be interpreted with caution and only used as part of an integrated approach that incorporates other patient characteristics, the clinical context, and local outcome data. Specific risk models also need to be developed for newer interventions, such as TAVI [Rosenhek R et al. Eur Heart J 2011].
- © 2011 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.