

Summary
Although data indicate that plaque modification does not have a direct influence on target lesion restenosis, it improves stent expansion and makes otherwise impossible cases possible. This article provides an overview of the need for devices to pretreat complex lesions with PM.
- interventional techniques & devices
- coronary artery disease
Calcified coronary lesions may be associated with stent underexpansion, malapposition, and high rates of restenosis. Aggressive plaque modification (PM) before stenting can reduce the risk of restenosis [Vaquerizon B et al. J Interv Cardiol 2010]. Although data indicate that PM does not have a direct influence on target lesion restenosis, it improves stent expansion and makes otherwise impossible cases possible. José F. Díaz, MD, Juan Ramon Jimenez University Hospital, Huelva, Spain, provided an overview of the need for devices that are currently available to pretreat complex lesions with PM.
There are several mechanical approaches that are available for PM. Some have been developed to ablate atheromatous plaque during percutaneous coronary interventions (PCIs), including the rotablator, cutting balloon, and a scoring device, which is similar to the cutting balloon.
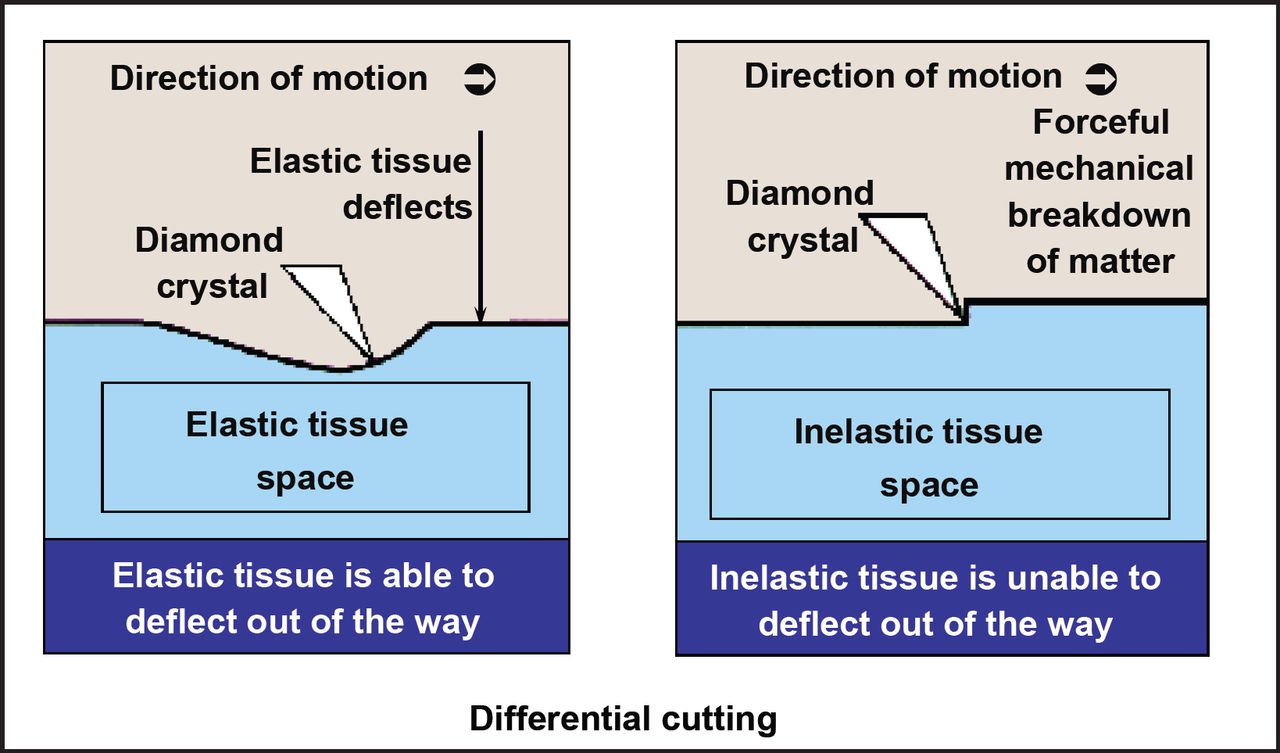
Rotational atherectomy is achieved using the diamond-headed rotablator, which employs differential cutting to remove inelastic tissue. Elastic tissue (healthy) is able to deflect out of the way of the rotablator and remains (Figure 1). The rotablator is best employed at medium rotational speeds (150,000 rpm) to polish the inside of the artery. This reduces platelet aggregation. This device should not be used in vessels with left ventricular dysfunction, vessels with extreme tortuosity, or saphenous vein grafts; where there is evidence of thrombus; for dissection; or in vessels with chronic total coronary occlusions. The rotablator has also not been proven to offer any advantages when used as a debulking device, at least regarding target vessel revascularization (TVR) or restenosis. However, it may be useful in situations in which there are heavily calcified lesions or the balloon is unable to cross/dilate the lesion.

Rotablator Principle of Operation.
Reproduced with permission from J. Diaz, MD.
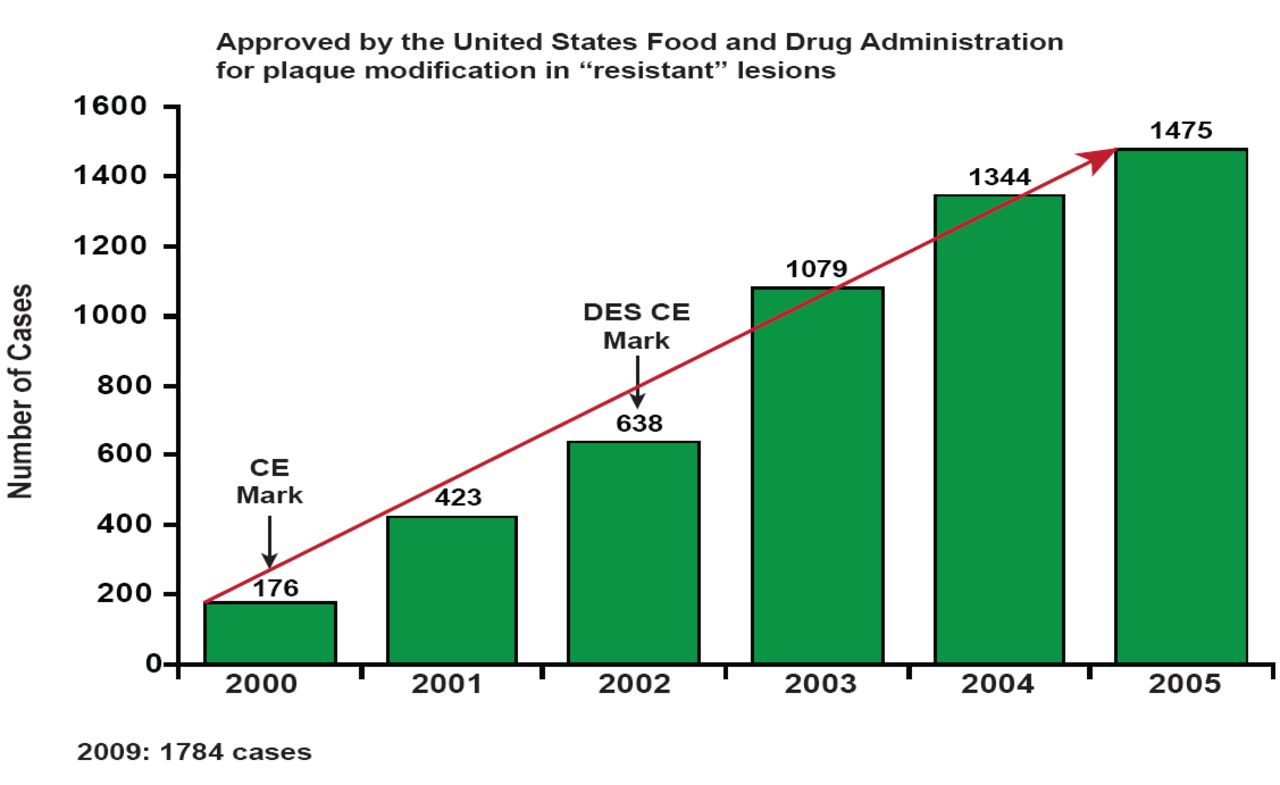
The cutting balloon consists of a noncompliant balloon with 3 to 4 cutting microtomes (a sectioning instrument that allows for the cutting of extremely thin slices) that are mounted on its surface, allowing for controlled cutting of the intima. Like the rotablator, the use of the cutting balloon is increasing in Spain (Figure 2). Like the rotablator, balloon cutting offers no clear advantages regarding rates of restenosis and TVR, but its use does result in less dissection, bailout stenting, balloon slippage, and plaque shifting. It may be particularly useful for small vessels, bifurcated vessels, ostial lesions, and in-stent restenosis. The major drawback is deliverability.

Cutting Balloon.
Reproduced with permission from J. Diaz, MD.
The third device, the scoring balloon, consists of 3 nitinol spiral “scoring” wires with nitinol-enhanced active deflation. It has a low crossing profile (2.7F) and is compatible with a 6F catheter or 5F sheath. It offers the advantages of being a nonslip device (avoids “geographic miss”), fewer dissections, fewer “snowplow effects” (pushing atherothrombotic material into a side branch or downstream), good deliverability, and having better stent expansion/apposition. One study has shown that pretreatment with the scoring balloon enhanced stent expansion and minimized the difference between predicted and achieved stent dimensions [De Ribamer Costa, Jr J et al. Am J Cardiol 2007]. In another study that was conducted in Israel (Israeli Registry), PM was performed with the scoring balloon prior to stent implantation in 745 patients. Procedural and clinical success rates were greater than 96%, device slippage occurred in only 1.2% of lesions, and there were no scoring balloon-related perforations.
Although early studies show the PM has little impact on the rate of restenosis, target lesion restenosis, or death rates and may increase procedural myocardial infarction and major cardiac adverse events [Bittl J et al. J Am Coll Cardiol 2004], Prof. Diaz believes PM may be important when dealing with selected acute cases. Specifically, it may help to decrease plaque volume and shifting, alter calcification, increase lesion compliance, facilitate stent delivery, and minimize vessel trauma.
- © 2011 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.