

Summary
A cost-effectiveness analysis of the Fractional Flow Reserve (FFR) Guided Percutaneous Coronary Intervention (PCI) Plus Optimal Medical Therapy (OMT) Versus OMT [FAME 2] trial indicates that FFR-guided PCI is economically viable. The initial cost of FFR-guided PCI is higher than that of medical therapy, but the cost gap narrows by >50% at 1 year.
- Cardiology Clinical Trials
- Interventional Techniques & Devices
- Coronary Artery Disease
A cost-effectiveness analysis of the Fractional Flow Reserve (FFR) Guided Percutaneous Coronary Intervention (PCI) Plus Optimal Medical Therapy (OMT) Versus OMT [FAME 2] trial indicates that FFR-guided PCI is economically viable. The initial cost of FFR-guided PCI is higher than that of medical therapy, but the cost gap narrows by >50% at 1 year, said William F. Fearon, MD, Stanford University, Stanford, California, USA, who presented the findings.
The FAME 2 trial showed that FFR-guided PCI plus OMT offered significant benefit compared with OMT alone for patients with stable coronary artery disease (CAD). The trial was prematurely stopped for significantly lower rates of hospitalization for urgent revascularization (p<0.001), but there was no difference in the rate of cardiovascular death or myocardial infarction [De Bruyne B et al. New Engl J Med 2012]. The study presented by Dr. Fearon was designed to determine if the benefits of FFR-guided PCI merited the costs.
The cumulative costs over 12 months were calculated. Angina was assessed at baseline, and 1, 6, and 12 months. Quality of life (QoL) was measured at baseline and 1 month (since the trial was stopped early) using the European quality of life-5 index scores with US weights. The researchers calculated the cost-effectiveness ratio for the first 12 months and projected the analysis out to 3 years. They assumed that the 1-year cost difference would persist in subsequent follow-up and the 1-month difference would decline linearly over 3 years.
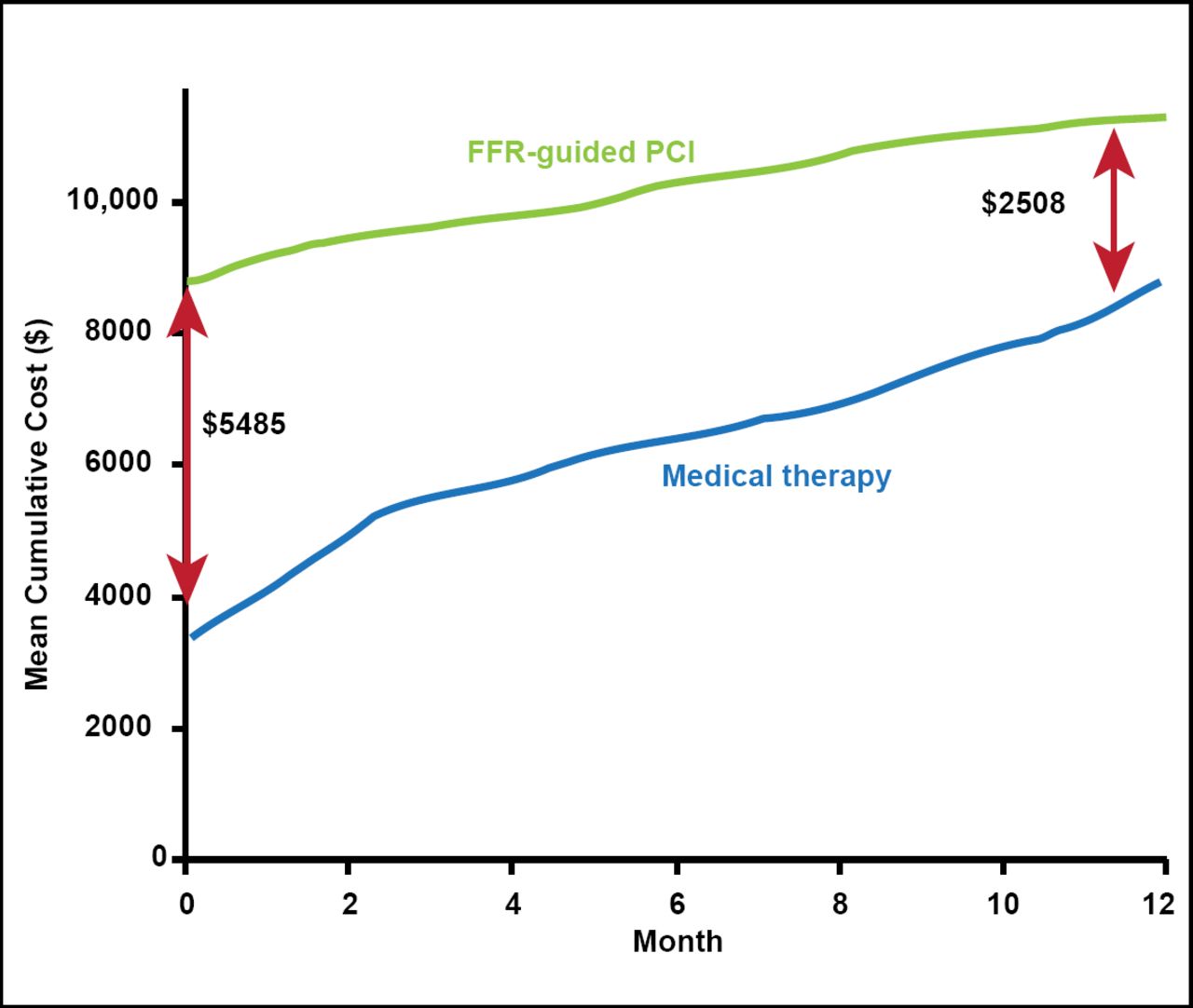
Dr. Fearon reported that the higher baseline cost for FFR-guided PCI ($8790 vs $3305 for medical therapy) was primarily related to the cost of drug-eluting stents (Table 1). The follow-up cost was higher for OMT ($5561 vs $2584 for FFR-guided PCI), with the higher cost primarily related to revascularization. The mean cumulative cost difference at baseline ($5485) decreased more than 50% at 1 year to $2508 (Figure 1). Dr. Fearon noted that the slope of the curves suggests that the cost gap would continue to narrow with further follow-up. He emphasized that (because the trial was stopped early) only a small percentage of the study population (11%) made up the cost estimate at 1 year, so the confidence limits were wide.
One Year Cost Estimates Per Patient.

Cumulative Costs over 12 Months.
Reproduced with permission from WF Fearon, MD.
With regard to QoL, significantly more patients in the FFR-guided PCI group were free of or had minimal angina (class 0 or 1) at 1 month (89% vs 71%; p<0.001). The change in the QoL score from baseline to 1 month increased 0.054 in the FFR-guided PCI group but was essentially unchanged (0.003) in the medical therapy group (p<0.001).
The in-trial cost-effectiveness ratio for FFR-guided PCI was $53,000 per quality adjusted life year (QALY). The 3-year projected cost-effectiveness was $32,000/QALY. To provide context for these ratios, Dr. Fearon explained that the traditional standard for hemodialysis cost-effectiveness is <$50,000/QALY. However, the benchmark is considered outdated by some, and the World Health Organization has suggested a new standard of three times the gross domestic product, which would be $150,000/QALY in the United States. Dr. Fearon said that a ratio between $50,000 to $150,000/QALY represents a debatable cost-effectiveness, but the 3-year projection of $32,000 is well below this benchmark.
The study's limitations include the short time horizon and the wide confidence limits of its cost-effectiveness estimates. However, FFR-guided PCI significantly improves angina and QoL compared with medical therapy, and it “appears to be economically attractive.”
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.