

Summary
This article discusses current insights into spondyloarthropathies, including TNF inhibition, structural damage progression in ankylosing spondylitis, methotrexate as a disease-modifying agent, and reactive arthritis.
- inflammatory disorders
TNF Inhibition and Structural Damage Progression in Ankylosing Spondylitis
Walter P. Maksymowych, MD, University of Alberta, Edmonton, Alberta, Canada, discussed the relationship between anti-TNF agents, inflammation, and lesions that demonstrate fat metaplasia in the structural progression of ankylosing spondylitis (AS).
Anti-TNF agents safely and effectively treat signs and symptoms of AS and improve health-related quality of life [Davis JC et al. Arthritis Rheum 2005; Lambert RG et al. Arthritis Rheum 2007]. Nonetheless, structural progression in AS has not been shown to be impacted by anti-TNF agents, despite the role of TNF-induced inflammation in the disease [van der Heijde D et al. Arthritis Rheum 2008]. This question has not been fully answered because of limitations in study design.
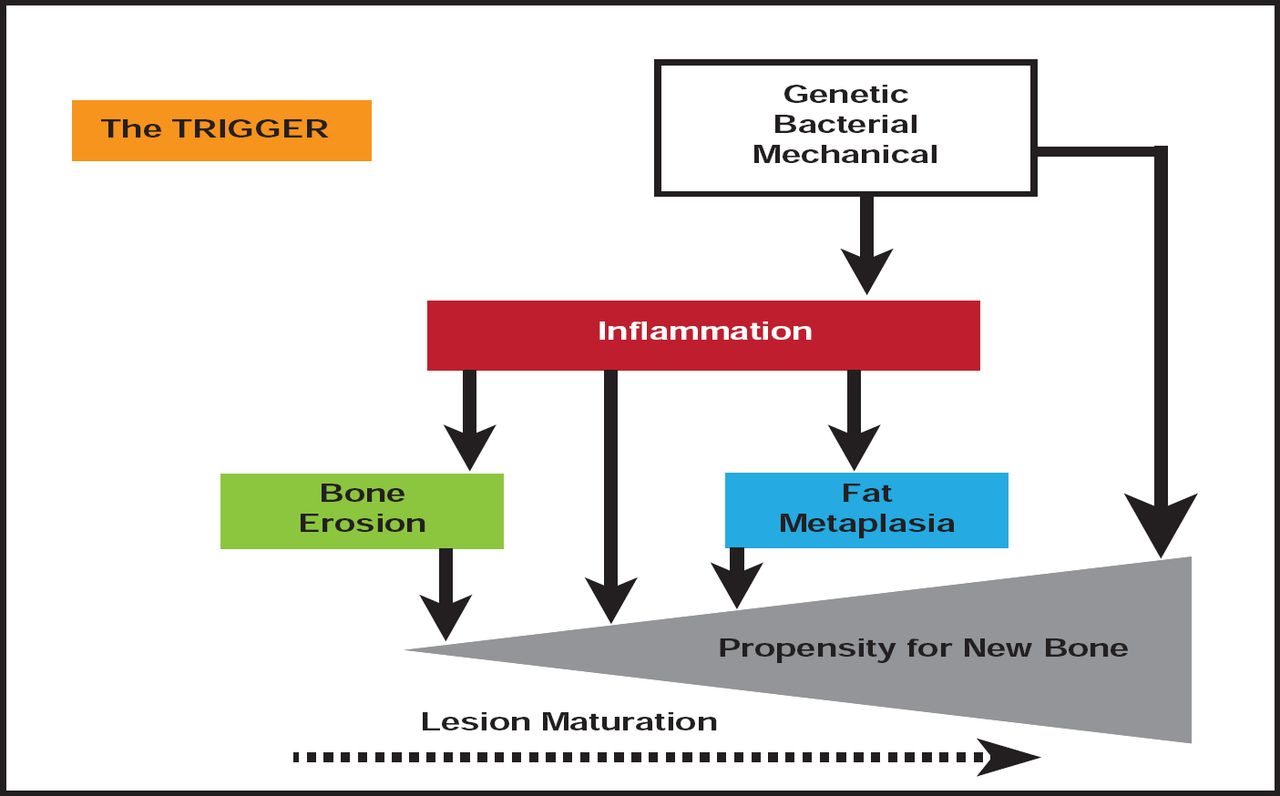
Questions persist over which MRI lesions predict the progression of AS. There is evidence that inflammatory lesions predict new bone formation, although the majority of new syndesmophytes develop at sites without active inflammation [Maksymowych et al. Arthritis Rheum 2009]. It has now been shown that inflammatory lesions that resolve undergo fat metaplasia and that this is associated with new bone formation. Fat metaplasia, therefore, appears to be an important intermediary in the pathway from inflammation to new bone (Figure 1) [Ann Rheum Dis 2011].

Pathogenesis of New Bone is Ankylosing Spondylitis.
Reproduced with permission from W. Maksymowych, MD.
PsA: Is Methotrexate a Disease-Modifying Agent?
Methotrexate (MTX) is often used as the primary treatment for psoriatic arthritis (PsA). However, there are limited data to demonstrate its clinical benefit, especially for axial disease [Gottlieb A et al. J Am Acad Dermatol 2008; Ritchlin CT et al. Ann Rheum Dis 2009; Gossec L et al. Ann Rheum Dis 2011]. Gabrielle H. Kingsley, MB, PhD, FRCP, Kings College, London, United Kingdom, discussed the role of MTX in the treatment of PsA, with a focus on whether MTX can be considered a disease-modifying antirheumatic drug (DMARD).
According to Prof. Kingsley, the aim of DMARD therapy is to improve long-term outcomes, not just symptoms. However, definitive demonstration of DMARD efficacy is difficult to confirm outside of placebo-controlled, randomized, controlled trials.
The MTX in Psoriatic Arthritis (MIPA) Trial [Kingsley et al. Rheumatology. In Press 2011] was a 6-month RCT that compared MTX with placebo to test the hypothesis that the drug improves disease activity and function in PsA. Key findings from the study indicate that MTX improves self-reported symptoms but has no effect on objective joint counts or acute phase reactants, which classifies it as a “symptom-modifying agent” rather than a DMARD. Prof. Kingsley recommends a reconsideration of current guidelines, based on new data [Baranauskaite A et al. Ann Rheum Dis 2011; Lie E et al. Ann Rheum Dis 2009; Kingsley GH et al. Rheumatology. In press 2011].
Reactive Arthritis: Clinical Insights and Treatment Options
Reactive arthritis (ReA) occurs 1 to 6 weeks after exposure to a causative organism, either postdysentery or postvenereal. John D. Carter, MD, University of South Florida, Tampa, Florida, USA, discussed the epidemiology of ReA and the pathophysiology, treatments, and outcomes of Chlamydia trachomatis-induced ReA (CiReA) [Carter JD et al. Arthritis Rheum 2009].
In the United States, the incidence of ReA is underestimated and underdiagnosed. Dr. Carter concluded that Chlamydia might be a common cause of undifferentiated spondyloarthropathies; that ocular serovars appear to be uniquely capable of causing ReA [Gerard HC et al. Microb Pathog 2010]; that ReA is a Th2-predominant disease; and that combination antibiotics show promise in the amelioration of CiReA symptoms and the elimination of the persistent state of Chlamydia.
- © 2011 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.