

Summary
In 1980, the recommendation from the Dietary Guidelines for Americans was to “avoid too much sodium.” Over time, however, formal guidelines have set ever-lowering intake goals, for which the scientific basis has become a matter of debate. Offering new snew perspectives on this controversy, this article discusses how dietary reference intakes are set, the relationship between sodium intake and cardiovascular disease, as well as population nutrition trends.
- nutrition physiology
- prevention & screening
In 1980, the recommendation from the Dietary Guidelines for Americans was to “avoid too much sodium.” Over time, however, formal guidelines have set ever-lowering intake goals, for which the scientific basis has become a matter of debate. Robert P. Heaney, MD, Creighton University, Omaha, Nebraska, USA, provided a new perspective on this controversy in his review of how dietary reference intakes (DRIs) are set.
In their 2005 guidelines, the Institute of Medicine (IOM) determined the adequate intake (AI) for sodium was 1500 mg/day for adults ≤ 50 years of age, 1300 mg/day for those aged 50 to 70 years, and 1200 mg/day for those aged >70, with an upper intake level (UL) for adults of 2300 mg/day [IOM. Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate. Washington, DC: The National Academies Press, 2005]. However, on May 14, 2013, IOM issued a new report concluding that salt intake in the range recommended by the earlier guidelines could increase the risk for heart-related illness and death and acknowledged that there was no evidence that reducing intake below 2300 mg/day was beneficial in terms of cardiovascular risk or mortality in the general population [IOM. Sodium Intake in Populations: Assessment of Evidence Washington, DC: The National Academies Press, 2013].
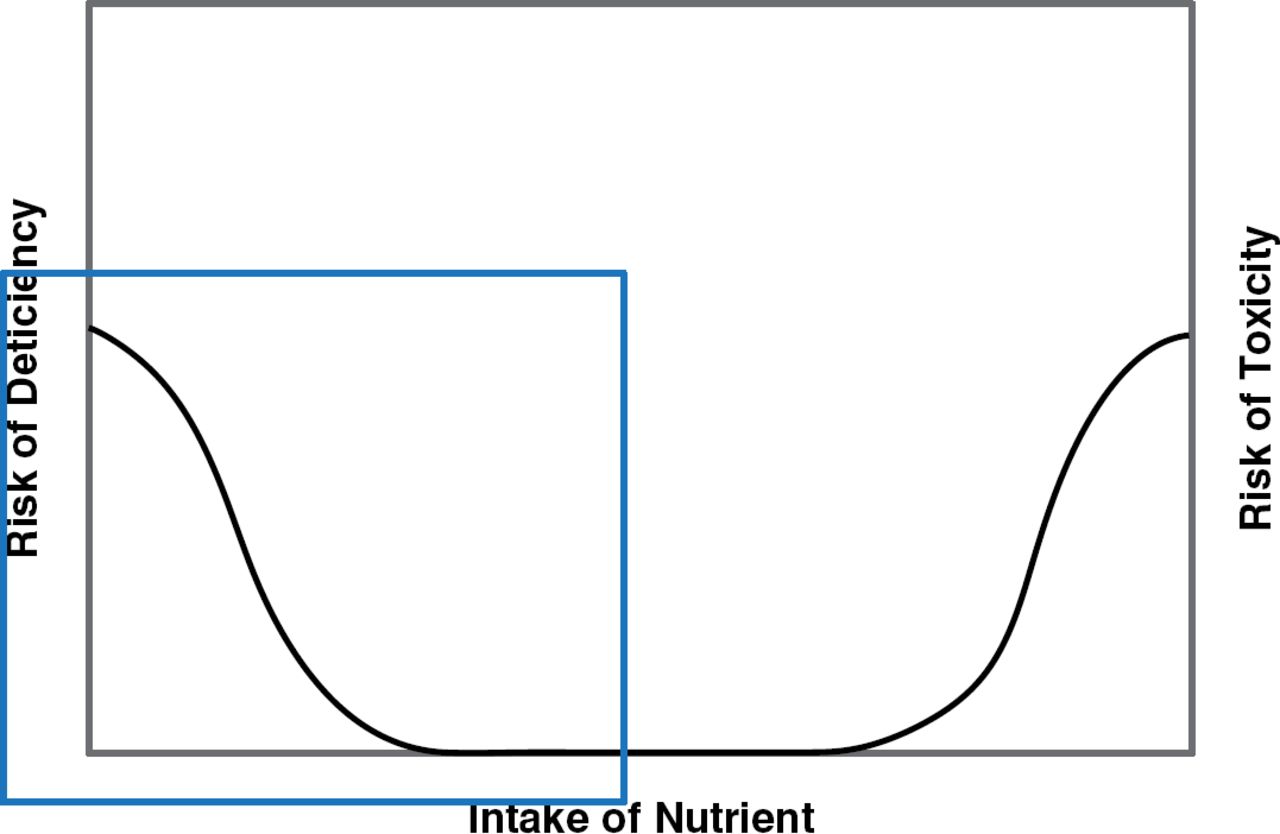
In theory, the process for calculating a DRI begins with identifying the consequences of inadequate and excessive intake of a nutrient. Next, the data describing the intake needed to avoid those consequences are gathered, and then an intake sufficient to avoid inadequacy is recommended. Most nutrient response curves are U-shaped with a risk of deficiency at the low end and risk of toxicity at the high end (Figure 1) [IOM. Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate. Washington, DC: The National Academies Press, 2005].

Nutrient Response and Intake Curve
Adapted from IOM. Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate. Washington, DC: The National Academies Press, 2005.
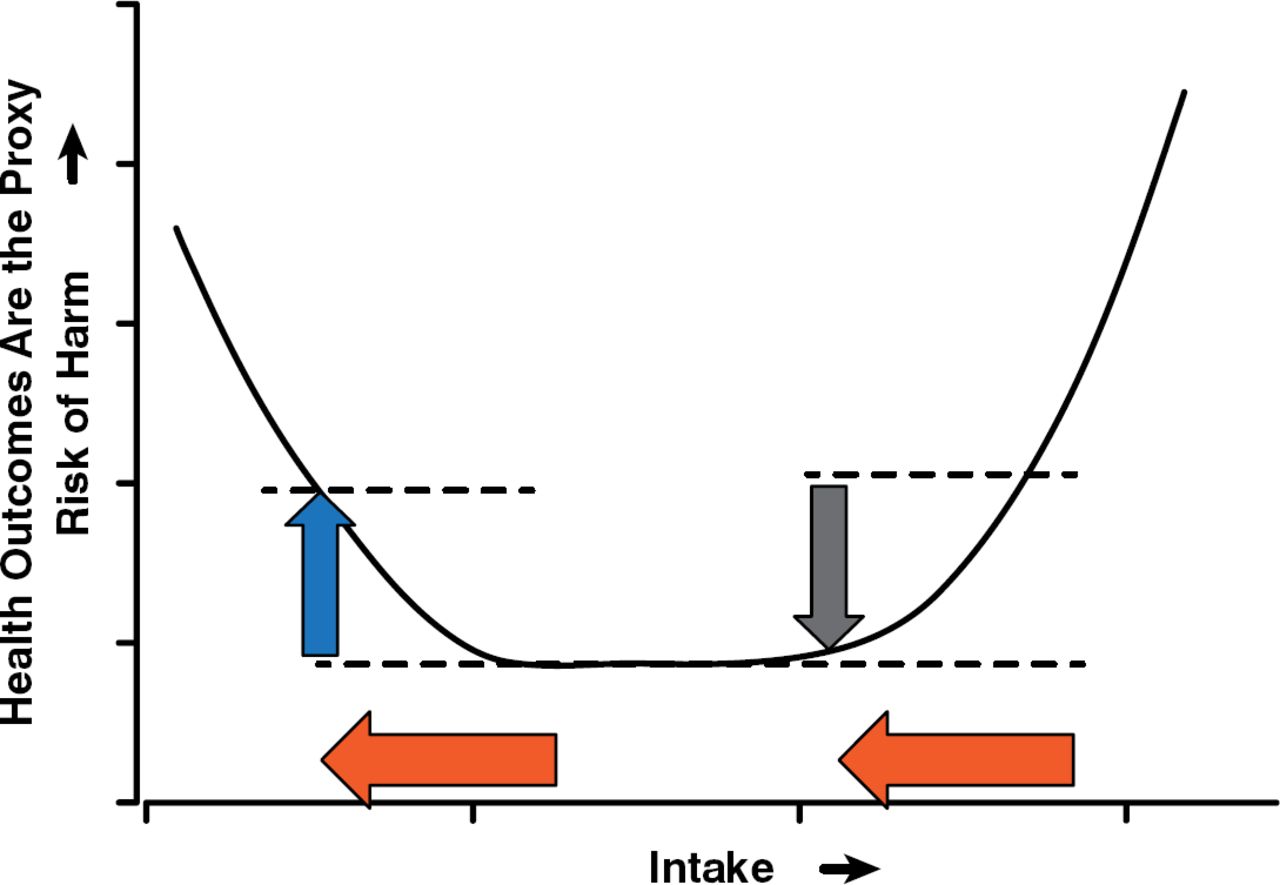
Because the IOM felt there was insufficient evidence regarding the effect of sodium to use the usual DRI process, they developed their 2005 recommendations based on adequate intake (AI), a concept defined as the average intake observed in a healthy population. The focus of a recommended intake is to avoid harm—not to create wellness—and the adverse effect the sodium intake guideline sought to avoid was elevated blood pressure (BP). By using an AI, the IOM took a linear approach, which did not account for the fact that the starting intake is an important consideration; ie, reductions from higher (toxic) levels of sodium intake would be expected to reduce risk, but reductions from lower levels may lead to an increase in risk (Figure 2).

The Importance of Starting Intake Levels
Reproduced with permission from RP Heaney, MD.
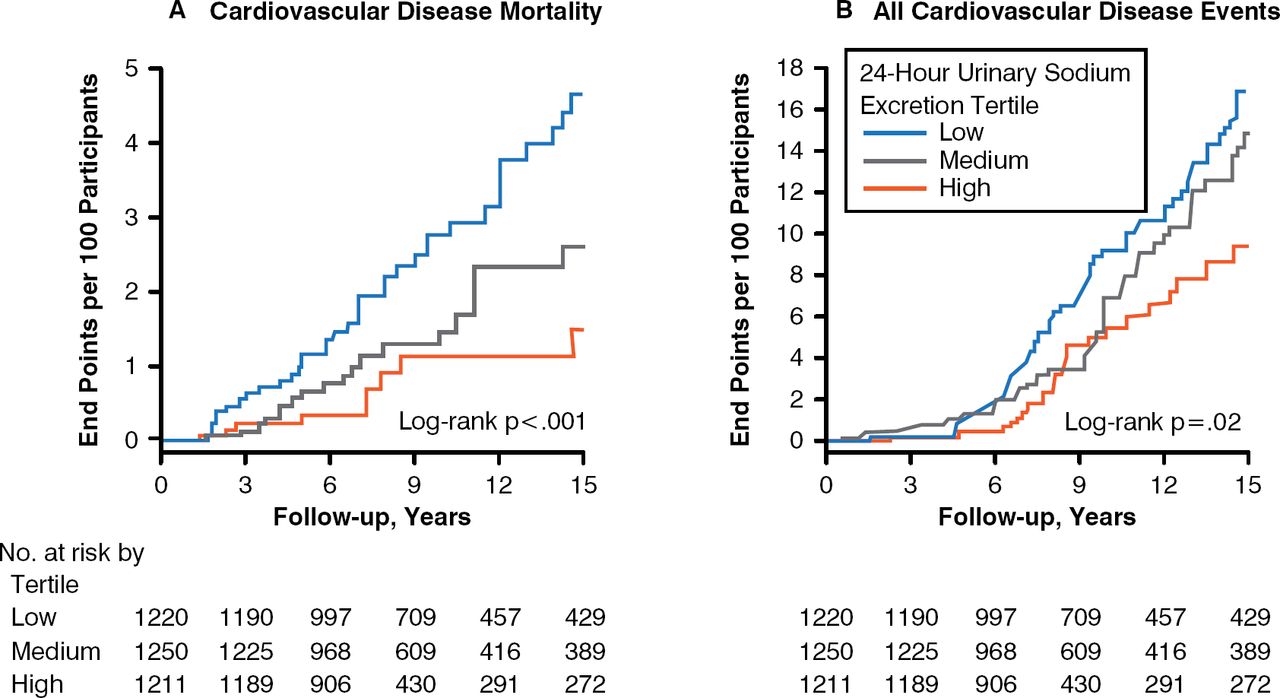
The relationship between sodium and cardiovascular disease (CVD) has been studied frequently but with inconsistent outcomes. Data from the National Health and Nutrition Examination Survey (NHANES) introduced questions about the sodium/BP connection 30 years ago when it was noted that higher intakes of calcium and potassium were associated with lower mean systolic BP and a lower absolute risk of hypertension. In a recent study, high urinary sodium excretion was not associated with increased CVD or mortality; however, low sodium excretion (in the range recommend by the 2005 guidelines) was associated with an increased risk of CVD morality (Figure 3) [Stolarz-Skzypek K et al. JAMA 2011]. In another study, the lowest CVD risk occurred between 4000 and 6000 mg/day of sodium excretion [O'Donnell MI et al. Eur Heart J 2013].

Cardiovascular Mortality and Morbidity and Sodium Intake
Reproduced from Stolarz-Skzypek K et al. Fatal and Nonfatal Outcomes, Incidence of Hypertension, and Blood Pressure Changes in Relation to Urinary Sodium Excretion. JAMA 2011;305(17):1777–1785. Copyright 2011 American Medical Association. All rights reserved.
The approach taken by the IOM in 2005 also failed to factor in the crucial roles of calcium and potassium intake. The classic Dietary Approaches to Stop Hypertension [DASH] studies revealed that higher intakes of calcium and potassium provided by certain foods can offset the negative effects of high sodium intake on BP. In the DASH diet, diets rich in fruits, vegetables, low-fat dairy foods with reduced saturated and total fat substantially lowered BP.
There are no randomized controlled trials (RCTs) regarding sodium intake, and the field lacks a consensus on how to define normal intakes, forcing reliance on empirical evidence. Dr. Heany proposes the use of the renin-angiotensin aldosterone system (RAAS) mechanism as a better benchmark rather than BP. Adjustments in the RAAS rescue for sodium becomes operative at sodium levels of ×3000 mg/day for an adult. Among hypertensive subjects, the plasma renin activity (PRA) level (without urine sodium), is independently and directly associated with the incidence of myocardial infarction (MI). For every 2-unit increase in PRA, there is an overall 25% increase in MI incidence.
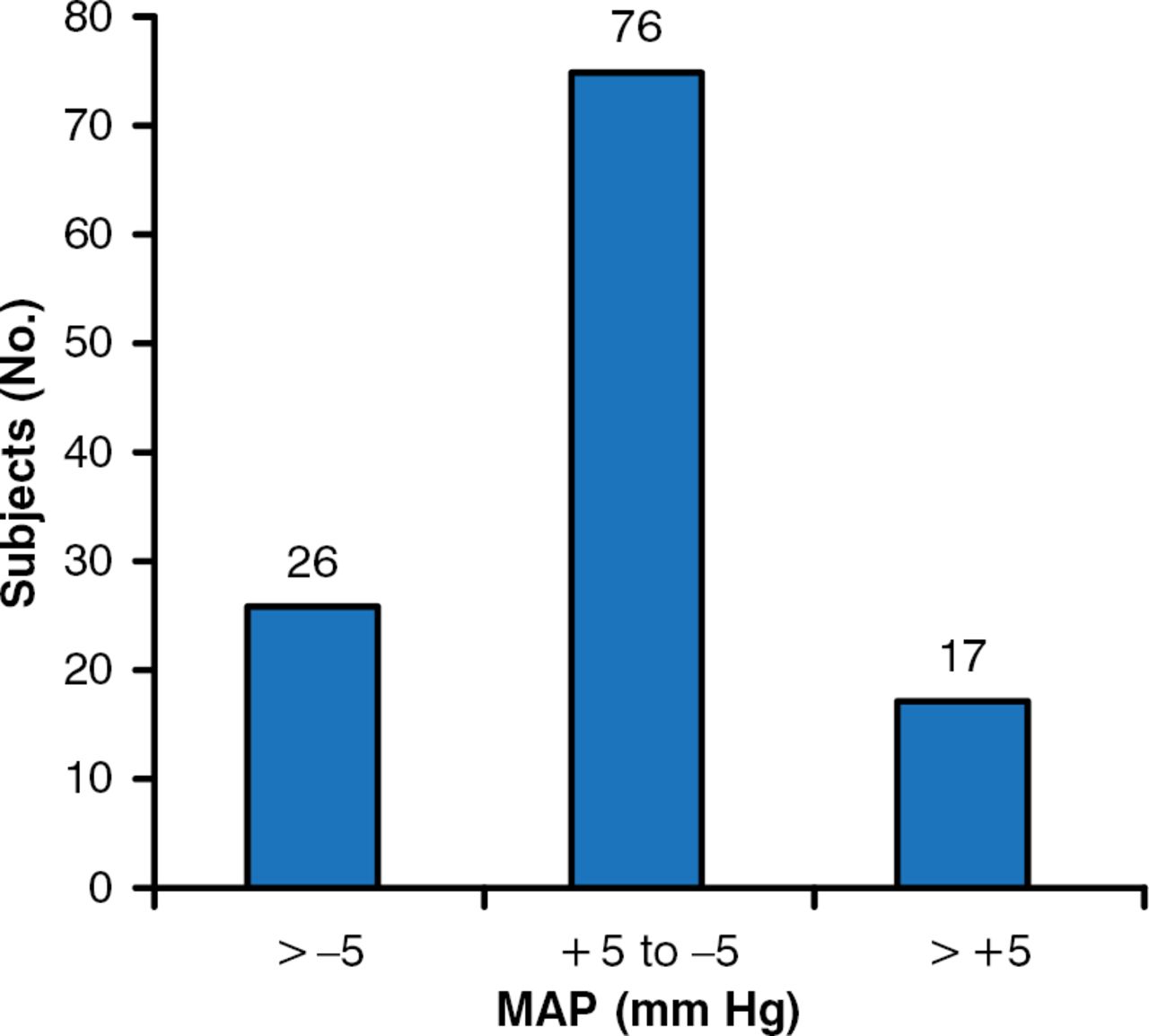
Continuing the discussion of sodium intake and health outcomes, Michael Alderman, MD, Albert Einstein College of Medicine, Bronx, New York, USA, noted that there are no precise data regarding dietary sodium intake and its relationship to CVD. Advocates argue that because lowering sodium reduces average BP (a CVD surrogate) it will prevent CVD. Skeptics argue that there are many physiological surrogates for CVD and altering only one does not assure a predictable CVD outcome. While it may make sense that reducing sodium intake will improve mortality by lowering BP, there is really no evidence. In several studies in the early 1980s, when investigators lowered sodium intake by significant amounts (≤ 70 mmol/day) most of the participants had no significant change in BP, some had a fall in BP, but BP in a substantial portion rose (Figure 4).

Heterogeneity of Blood Pressure Response in 119 Mild Hypertensive Subjects
MAP=mean arterial pressure.
Sources: Longworth DL et al. Clin Pharmacol Titer 1980; MacGregor GA et al. Lancet 1982; Watt G et al. Br Med/1983.
Reproduced with permission from M Alderman, MD.
Reducing sodium intake has multiple physiological effects both positive and negative, and the health outcome is not predicted by one effect alone but by a network of multiple effects. Multiple RCTs support a “J-shaped” relationship between sodium and CV outcomes such that intakes below 2500 mg/day or above 6000 mg/day are associated with increased CV risk [Alderman MH, Cohen HW. Curr Hypertens Rep 2012].
The 2013 IOM report did not recommend an optimal range for sodium intake. However, a very recent meta-analysis investigating the association between sodium intake and health outcomes among 275,000 subjects with low, usual, or high sodium intakes found that a range of 2645 to 4945 mg/day was associated with the most favorable outcomes [Graudal N et al. Am J Hypertens 2014]. This compares favorably with the sodium consumption of 90% of Americans, which is between 2500 and 5000 mg/day.
Guidelines calling for strict reductions in sodium are based on the premise that intake exceeds physiological need and that it can and should be reduced for optimum health. David McCarron, MD, University of California, Davis, Davis, California, USA, discussed data supporting the consistency of sodium intake over time and across populations despite public policy efforts to reduce it.
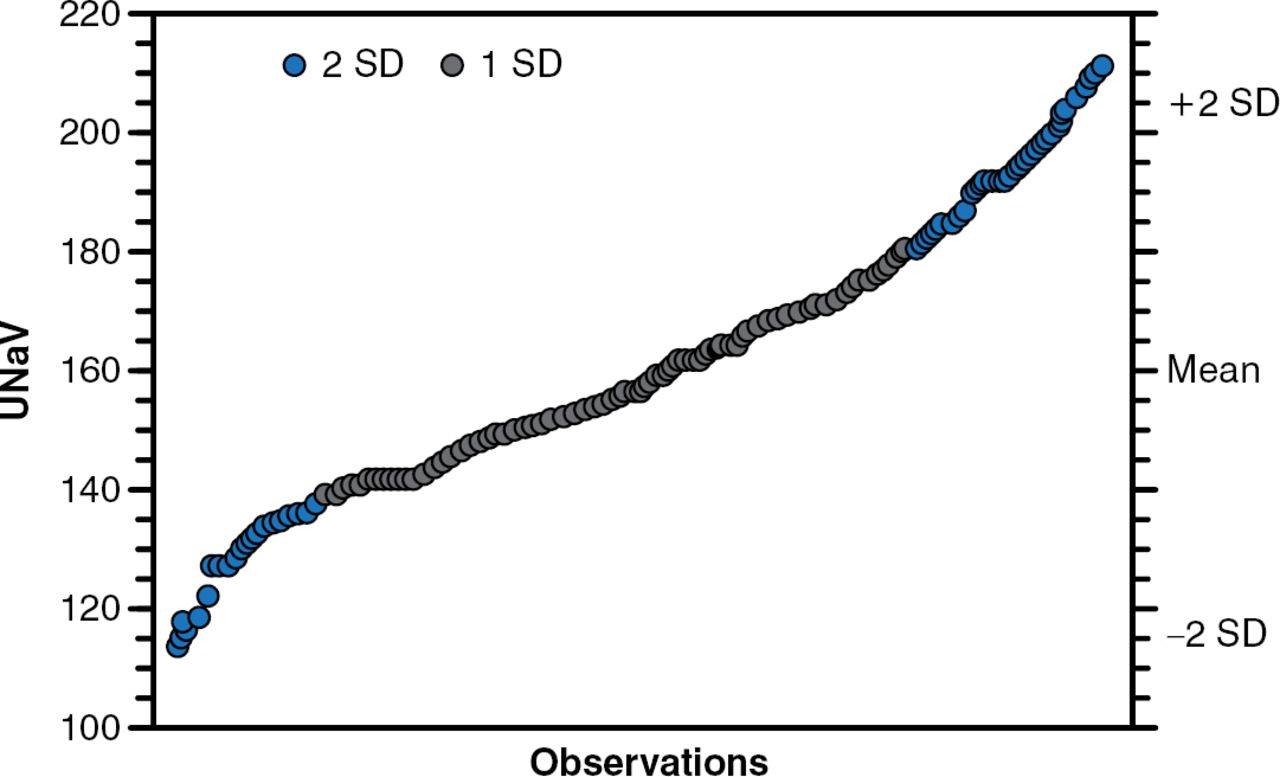
Neuroscientists have identified neural circuits in vertebrate animals that regulate sodium appetite within a narrow physiological range, and that sodium appetite is controlled by physiological need rather than environmental factors [McCarron DA et al. Am J Hypertens 2013]. The intake range is remarkably reproducible over at least 5 decades across 45 countries (Figure 5).

Range of Human Sodium Intake Worldwide
SD=standard deviation; UNaV=urinary sodium excretion.
Based on 24-hour UNaV in 69,011 subjects worldwide; 5 decades, 45 countries; mean: 159.4 ± 22.3 mmols/day; range: 114–210 mmols/day (2622–4830 mg/day).
Reproduced from McCarron DA et al. Normal Range of Human Dietary Sodium Intake: A Perspective Based on 24-Hour Urinary Sodium Excretion Worldwide. Am J Hypertens 2013;26(10):1218–1223. With permission from Oxford University Press.
The range has definable upper and lower limits with health risks at each end; the mid-range values are associated with optimal health benefits. Intake is controlled by various stimulatory and inhibitory signals that act on the brain to regulate sodium appetite; it is not primarily determined by food. For instance, sodium appetite can be enhanced by the adrenal steroid aldosterone via an unknown brain mechanism [Geerling JC et al. J Neurosci 2006].
Dr. McCarron presented evidence showing the normal range of human sodium intake and that the intake in the United States is within that range. Future guidelines should be based on this biologically determined range of approximately 2500 to 5000 mg/day.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.