

Summary
In any given year, 26.2% of individuals in the United States experience a diagnosable psychiatric illness. Approximately 6% of adults suffer from a seriously debilitating mental illness. Among adolescents aged 13 to 18 years, 46.3% experience symptoms of psychiatric illness, and 21.4% experience a severe disorder. This article discusses clinical tools for personalizing psycho-pharmacologic treatment, including psychopharmacogenetics, laboratory studies, review of systems, symptom evaluation, and observation.
- psychopharmacology
In any given year, 26.2% of individuals in the United States experience a diagnosable psychiatric illness [National Institute of Mental Health. 2012]. Approximately 6% of adults suffer from a seriously debilitating mental illness. Among adolescents aged 13 to 18 years, 46.3% experience symptoms of psychiatric illness, and 21.4% experience a severe disorder. In this presentation, Laura G. Leahy, DrNP(c), APRN, APNSolutions, LLC, Sewell, New Jersey, USA, presented real-life prescriptive challenges in treating patients with psychiatric illnesses and offered innovative ways to address them. She discussed clinical tools for personalizing psychopharmacologic treatment, including psychopharmacogenetics, laboratory studies, review of systems, symptom evaluation, and observation.
CASE STUDY AND PERSONALIZED TREATMENT
Ms Leahy presented the case of a boy, aged 8 years, with symptoms of restlessness, fidgeting, inattention, poor sleep, limited appetite, forgetfulness, frustration, and decreasing grades. He was diagnosed with attention-deficit/hyperactivity disorder (ADHD) and was prescribed an extended-release psychostimulant by his pediatrician. The restlessness and fidgeting initially improved, but the patient developed an upset stomach and headaches, and his grades continued to decrease. The psychostimulant was discontinued, and the physical and behavioral symptoms continued. Results of a full medical workup and computed tomography scan of the brain were normal, so he was referred to a psychiatric mental health nurse practitioner (PMHNP), who started him on a trial of the selective norepinephrine reuptake inhibitor (SNRI) atomoxetine.
Many factors influence the development of psychiatric illness, including genetic, epigenetic, developmental, and environmental factors. These factors should be considered when evaluating and treating patients.
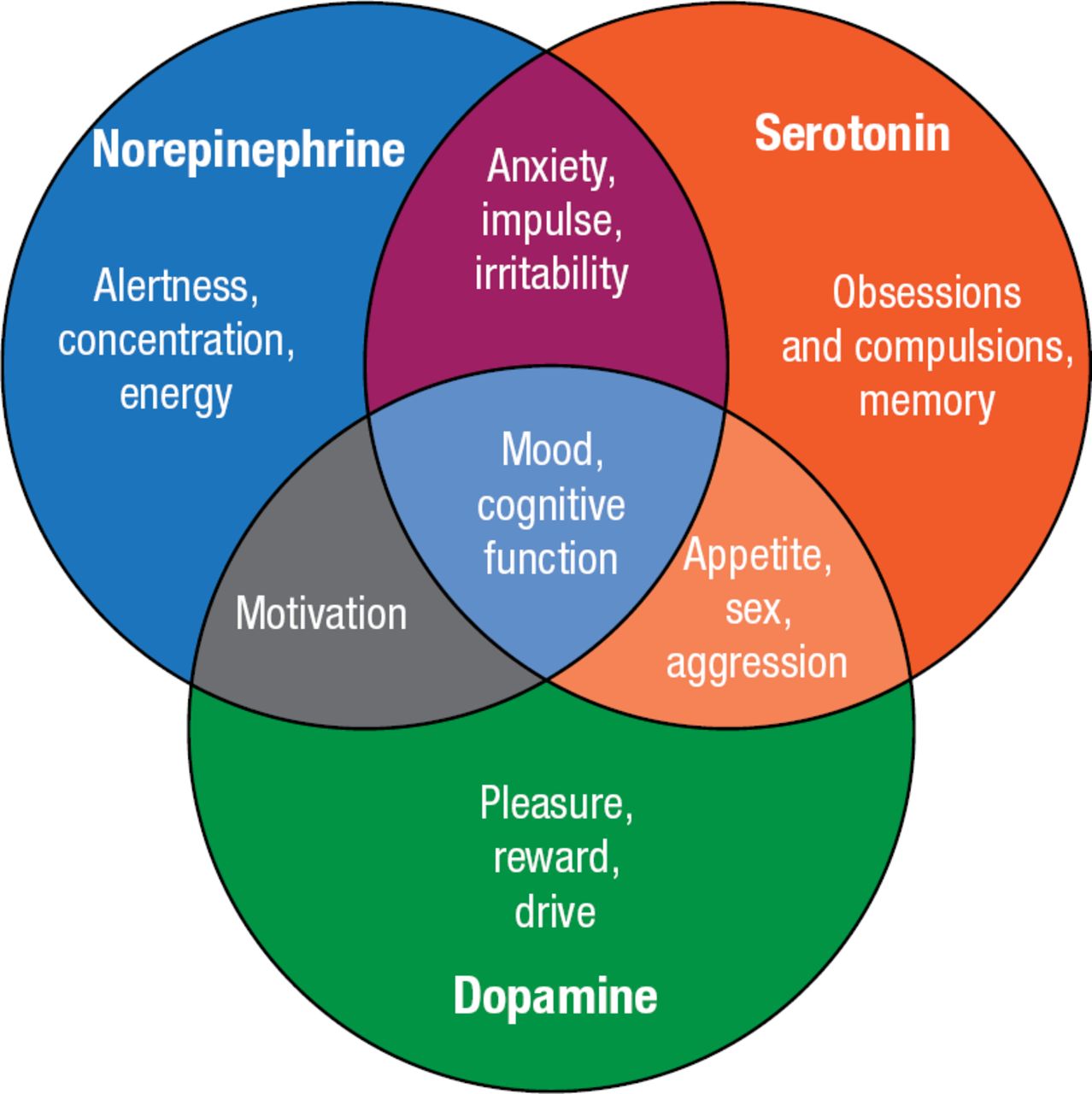
According to Ms Leahy, the use of observation, education, clinical testing, and nursing experience leads to improved decision making and patient outcomes. A complete evaluation includes a review of systems and laboratory studies, including complete blood count, electrolytes and metabolic panel, and hormone and vitamin-level testing. Neurotransmitter levels are also important, as they affect mood and mental function (Figure 1).

Effects of Neurotransmitters
Reproduced with permission from LG Leahy, DrNP(c).
Adapted from Healy D et al. The enhancement of social functioning as a therapeutic principle in the management of depression. J Psychopharmacol. 1997;11:S25-S31. With permission from British Association for Psychopharmacology.
Norepinephrine and dopamine deficiencies are associated with ADHD. A deficiency of norepinephrine contributes to inattention and elevated anxiety responses. Dopamine deficiency is associated with poor concentration, inattention, and inability to regulate inhibitions.
The case study patient stayed on atomoxetine, and his symptoms were in remission through middle school. However, by age 14, he was missing occasional doses of atomoxetine and developed symptoms of agitation, irritability, defiance, and sleep fluctuations from hypersomnolence to insomnia. Family therapy was started, but after 3 months, his symptoms worsened. A review of the family history revealed that the patient's paternal grandfather suffered from manic depression and alcoholism and his paternal uncle committed suicide in his mid-20s. Pharmacogenetic testing, via the Genecept salivary assay ordered by the PMHNP, revealed that the patient had the following gene variants: 5-HT2C C/C, CACNA1C G/A, COMT Val/Val, MTHFR C/T, and CYP2D6 IM/PM. The implications of these gene variants and others associated with psychiatric illness are shown in Table 1.
Genotypes and Implications for Personalized Medicine
On the basis of his genotype, the patient was prescribed lithium and L-methylfolate. From ages 19 to 21, the patient abruptly discontinued all of his medications. He began drinking on weekends and weeknights and smoking marijuana to “help him sleep.” When drinking, he became angry and aggressive. After failing his first year of college and getting arrested for driving under the influence, he agreed to return to the PMHNP. Because the patient hated the blood draws necessary with lithium, the PMHNP started a trial of gabapentin, which was consistent with his genotype. Recent studies demonstrated the efficacy of gabapentin for alcohol and marijuana abstinence and as a sleep aid.
PSYCHOPHARMACOLOGY
Personalized pharmacologic treatment of psychiatric illness involves selecting therapies based on a patient's history, clinical features, laboratory and other studies, genotype, and potential adverse effects of medications. Approximately 50% to 60% of patients benefit from their first medication trial; 30% to 50% benefit from their second medication trial [Trivedi MH et al. Am J Psychiatry. 2006]. Approximately 25% to 33% of patients do not respond after > 3 trials with adequate medication and are considered treatment resistant.
Many psychotropics are associated with significant adverse effects, such as an increased risk of mortality in elderly patients with dementia using atypical antipsychotics [US Food and Drug Administration. www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm124830.htm. Accessed December 24, 2014]; increased suicidality in children, adolescents, and young adults using antidepressants [US Food and Drug Administration. www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/UCM096273. Accessed December 24, 2014]; and a risk of sudden death and cardiovascular events and potential for abuse and dependence with psychostimulants [US Food and Drug Administration. www.fda.gov/Drugs/DrugSafety/ucm277770.htm. Accessed December 24, 2014]. Atomoxetine, duloxetine, nefazodone, and pemoline have the potential to cause severe hepatotoxicity [United States Food and Drug Administration. MedWatch Safety Alerts for Human Medical Products. 2005]. Care must be taken when treating women of childbearing age, as most of the therapies are not approved for use in pregnancy and may have teratogenic effects. However, serotonin selective reuptake inhibitors (SSRIs) have been used successfully during pregnancy. Most medications are not approved for children, but many have a long successful history of use in children. The dose of and duration on medication should be maximized in children who have some response. With elderly patients, a thorough medical and medication history should be taken. Doses may need to be lowered due to slower liver metabolism, and adverse effects should be closely monitored.
Treatment options include combination and augmentation strategies, such as lithium, triiodothyronine, and stimulants; atypical antipsychotic agents; omega-3 fatty acids and L-methylfolate; modafinil and stimulants; and lamotrigine. Patients with treatment-resistant symptoms may be switched between an SSRI and an SNRI (symptoms: alteration in concentration, energy, fatigue, anxiety, impulsivity, memory, or irritability); an SSRI and a norepinephrine-dopamine reuptake inhibitor (NDRI; symptoms: alteration in motivation, pleasure, aggression, sexual dysfunction, weight, memory, or obsessions and compulsions); or an SNRI and an NDRI (symptoms: alteration in energy, alertness, concentration, attention, pleasure, or motivation). Table 2 lists the drug classes used for psychiatric illnesses and their key features.
Drug Classes and Key Features
Ms Leahy concluded that the holistic approach to treatment of patients with psychiatric symptoms helps to identify potential medical mimics and other nonpsychiatric conditions. Moving into the 21st century, PMHNPs must integrate their powers of observation with concepts of advanced neuroscience, brain chemistry and pathology, and pharmacogenetics and partner with their patients to develop a “tool kit” to improve their quality of life.
- © 2015 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.