

Summary
An estimated 13.5% of global premature deaths and 54% of strokes are attributable to hypertension. Therefore, the topic of adequate blood pressure (BP) control is important, and as of 2012, the BP goals have changed. This article discusses the Kidney Disease: Improving Global Outcomes (KDIGO) organization, the 2013 ESH/ESC guidelines for the management of arterial hypertension, 2014 JNC 8 and ASH/ISH guidelines, as well as how to integrate the hypertension guidelines into clinical practice.
- Hypertensive Disease Cardiology Guidelines
- Hypertension & Kidney Disease
- Cardiology
- Hypertensive Disease
- Nephrology
- Cardiology Guidelines
- Hypertension & Kidney Disease
- Cardiology
An estimated 13.5% of global premature deaths and 54% of strokes are attributable to hypertension [Lawes CM et al. Lancet. 2008]. Therefore, the topic of adequate blood pressure (BP) control is important, and as of 2012, the BP goals have changed. George L. Bakris, MD, University of Chicago, Chicago, Illinois, USA, discussed the Kidney Disease: Improving Global Outcomes (KDIGO) organization, founded in 2003, and the rationale behind the BP goal. The mission of KDIGO is to coordinate and collaborate to develop and implement clinical practice guidelines for kidney disease to improve worldwide outcomes.
The seventh Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) and the American Diabetes Association (ADA) in 2003, as well as the National Kidney Foundation (NKF) in 2000, stated that the BP goal for patients with chronic kidney disease (CKD) should be < 130/80 mm Hg. In 2012, the KDIGO/NKF Kidney Disease Outcomes Quality Initiative (KDOQI) guideline increased the BP goal to < 140/90 mm Hg, as did a 2014 Expert Panel, and similar to the ADA increase in 2013 to < 140/80 mm Hg.
Higher systolic blood pressure (SBP) is associated with decreased glomerular filtration rate (GFR); Dr Bakris shared data compiled from numerous studies showing patients with CKD achieve SBPs > 130 or even > 140 mm Hg. In the MDRD study, patients with a mean arterial pressure of < 107 mm Hg were more likely to experience kidney failure sooner than patients with a lower mean arterial pressure of < 92 mm Hg over 12 years of follow-up [Sarnak MJ et al. Ann Intern Med. 2005]. In the REIN-2 study, although the intensified control arm achieved considerable separation in mean arterial pressure from the conventional control arm, a similar number of patients without diabetic nephropathy in the 2 arms experienced end-stage renal disease [Ruggenenti P et al. Lancet. 2005]. There are no randomized controlled trials that have evaluated the effect of BP goals in patients with diabetic nephropathy.
The 2012 KDIGO/2013 KDOQI guidelines recommend lifestyle modifications as part of the management to lower or maintain BP [Taler SJ et al. Am J Kidney Dis. 2013; Wheeler DC, Becker GJ. Kidney Int. 2013]. For adults with or without diabetes with albuminuria < 30 mg/24 h, the treatment goal is < 140/90 mm Hg; for patients with or without diabetes with albuminuria > 30 mg/24 h, the goal is < 130/80 mm Hg. Angiotensin receptor blockers (ARBs) and angiotensin-converting enzyme inhibitors (ACE-Is) are suggested as initial therapy for those patients with albuminuria and without diabetes who require treatment to reduce or maintain BP. Adult patients who have received a kidney transplant should maintain a BP < 130/80 mm Hg. Pediatric patients should receive BP-lowering agents when their BP is consistently > 90th percentile for age, sex, and height, to a goal that is ≤ 50th percentile for age, sex, and height without causing hypotension.
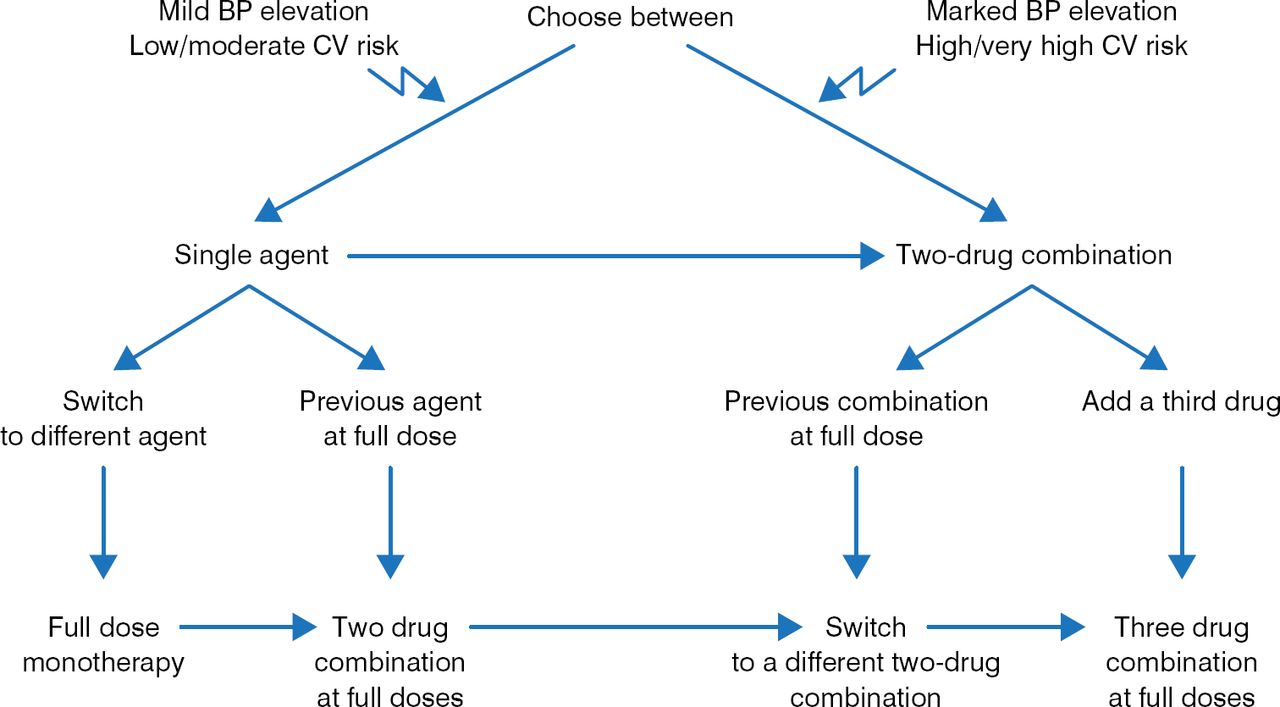
Luis M. Ruilope, MD, PhD, Complutense University, Madrid, Spain, discussed the 2013 European Society of Hypertension (ESH)/European Society of Cardiology (ESC) guidelines for the management of arterial hypertension [Mancia G et al. J Hypertens. 2013]. This guideline defines hypertension as > 140/90 mm Hg. However, patients with CKD are considered to be at moderate to high risk beginning at 130/85 mm Hg, and CKD is recognized as a risk factor that affects prognosis. The ESH/ESC guidelines recommend that lifestyle modifications be initiated in patients with CKD with high-normal SBP or diastolic BP. In addition, monotherapy and combination therapy can be used to achieve the target B P, with single therapy used primarily in patients with mild BP elevation (Figure 1).

Schema for Treatment of Elevated BP
BP, blood pressure; CV, cardiovascular.
Reprinted from Mancia G et al. 2013 ESH/ESC Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2013;31:1281–1357. With permission by Wolters Kluwer Health | Lippincott Williams & Wilkins.
Potential combinations include thiazide diuretics, ARBs, calcium antagonists, ACE-Is, β-blockers, and other antihypertensive agents. For elderly patients, the BP goal is < 140 mm Hg for those who are fit and aged < 80 years; for elderly patients with an initial SBP of ≥ 160 mm Hg, the goal should be 140 to 150 mm Hg. Frail elderly patients should be treated according to the discretion of the physician, based on the effects of treatment. For patients with diabetes, nephropathy, cerebrovascular disease or history of stroke or transient ischemic attack, and chronic heart disease, the BP goal is < 140/85 mm Hg. For patients with resistant hypertension, any agent that has a lack of effect should be discontinued, and other agents such as mineralocorticoid receptor antagonists, amiloride, and α1-blockers considered, as well as invasive approaches such as renal denervation and baroreceptor stimulation if pharmacotherapy fails.
Sandra J. Taler, MD, Mayo Clinic, Rochester, Minnesota, USA, discussed the 2014 JNC 8 and American Society of Hypertension (ASH)/International Society of Hypertension (ISH) guidelines. The 2014 JNC 8 guidelines recommend that patients aged ≥ 60 years should have a target BP of < 150/90 mm Hg, and patients with CKD or diabetes should have a target of < 140/90 mm Hg [James PA et al. JAMA. 2014]. The preferential initial treatment to reduce BP, if the patient is not black, is a thiazide-type diuretic, a calcium channel blocker, an ARB, or an ACE-I. For black patients, the first choice is a thiazide-type diuretic or calcium channel blocker, and for patients with CKD, an ARB or ACE-I. The combination of an ARB with an ACE-I should be avoided. Other agents that can be added to initial therapy include spironolactone or amiloride, α-blocker, β-blocker, vasodilator, α-β-blocker, and a central agonist.
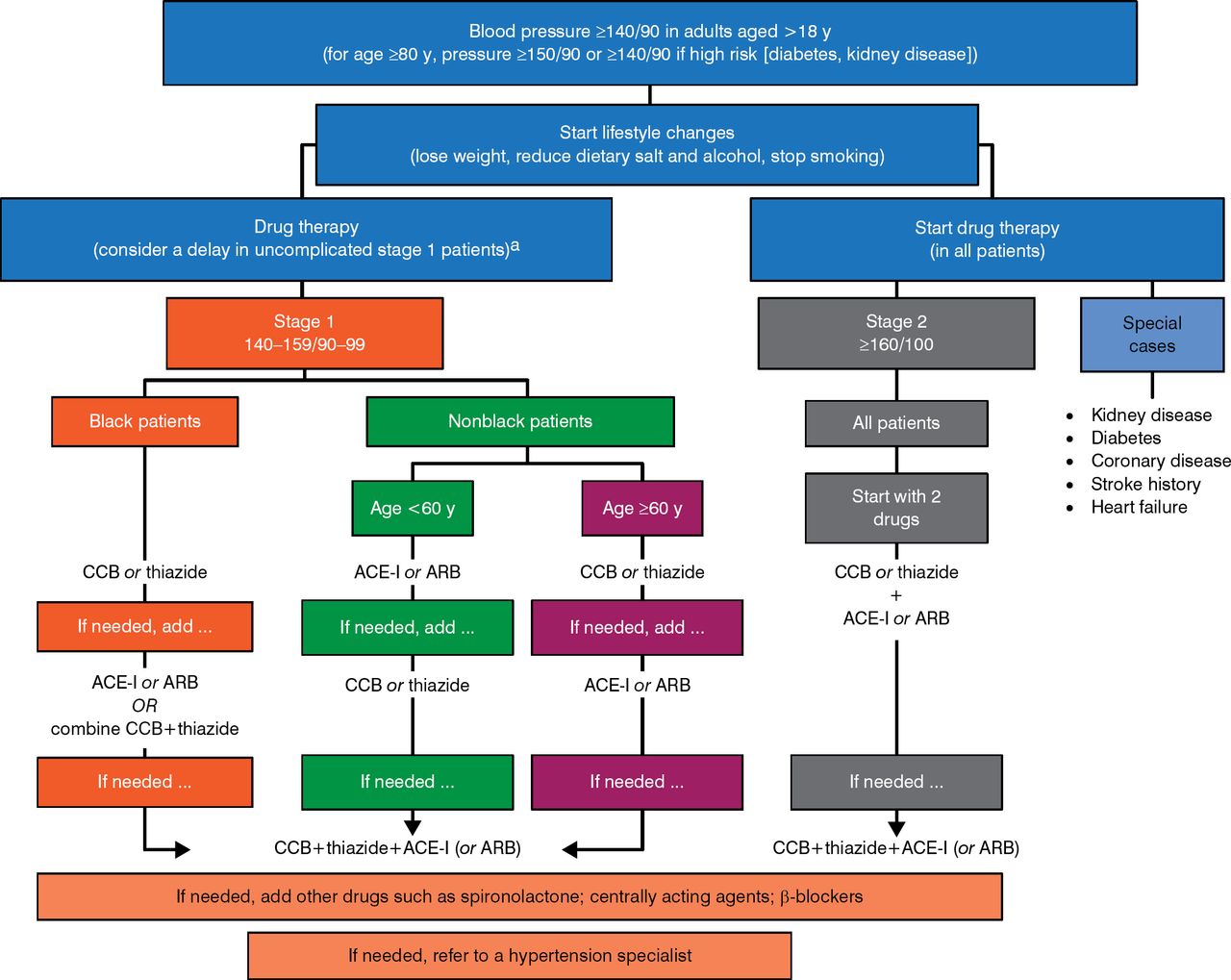
The 2014 ASH/ISH guideline was designed for primary care practitioners and students so that patients in all locations could receive professional hypertension care [Weber MA et al. J Clin Hypertens (Greenwich). 2014]. Overall, the BP targets and therapies are similar to those recommended in the JNC 8 guidelines (Figure 2). However, the recommendations of the ASH-ISH guidelines are primarily based on expert opinion, whereas the JNC 8 guideline is evidence based, albeit of limited scope.

2014 ASH/ISH Schema for Blood Pressure Reduction
ACE-I, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; CCB, calcium channel blocker.
aIn stage 1 patients without other cardiovascular risk factors or abnormal findings, some months of regularly monitored lifestyle management without drugs can be considered.
Adapted from Weber MA et al. Clinical Practice Guidelines for the Management of Hypertension in the Community: A Statement by the American Society of Hypertension and the International Society of Hypertension. J Clin Hypertens. 2014;16:14–26. With permission from John Wiley & Sons, Inc.
Matthew R. Weir, MD, University of Maryland School of Medicine, Baltimore, Maryland, USA, described how to integrate the hypertension guidelines into clinical practice. The goal of BP lowering in patients with CKD is to prevent cardiovascular disease (CVD) events and to prevent further deterioration of GFR. In patients with CKD, lower GFR is associated with a greater risk of experiencing a CVD event [Shastri S, Sarnak MJ. Am J Kidney Dis. 2010]. In addition, patients with CKD, particularly those with CKD and diabetes, are at a greater risk of death [Collins AJ et al. Kidney Int. 2003].
Hypertensive renal damage is influenced by BP load, transmission or intrarenal pressures, and susceptibility mechanisms including structural and functional differences. Patients who achieve lower SBP goals are less likely to reach doubling of serum creatinine levels or end-stage renal failure compared with patients with higher BP.
Dr Weir argued that the word hypertension has no real meaning; instead, clinicians should establish a BP goal for individual patients based on their benefit-to-risk ratio for the pharmacologic intervention. He also emphasized that when evaluating results from a study, it is important to consider factors such as the level of renal function, albuminuria, and trial design.
There are multiple guidelines for the management of patients with hypertension, with some differences in recommended BP goals and initial therapies. It is important to remember that patients are individuals, and no two are alike when determining a given patient's BP goals and potential BP reduction therapy.
- © 2015 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.