

Summary
Magnetic resonance imaging (MRI) and standing lateral and flexion-extension (SLFE) radiographs should be obtained in patients thought to have L4-L5 lumbar degenerative spondylolisthesis (LDS). This article presents the results of a retrospective imaging study to determine the sensitivity of MRI in diagnosing LDS and whether L4-L5 facet joint effusions predicted LDS.
- Orthopaedics Clinical Trials Spine Conditions
- Radiography
- Orthopaedics Clinical Trials
- Orthopaedics
- Spine Conditions
- Radiography
Magnetic resonance imaging (MRI) and standing lateral and flexion-extension (SLFE) radiographs should be obtained in patients thought to have L4-L5 lumbar degenerative spondylolisthesis (LDS). Benjamin D. Kuhns, MS, The Cleveland Clinic, Cleveland, Ohio, USA, presented the results of a retrospective imaging study [Kuhns BD et al. Spine J. 2014] to determine the sensitivity of MRI in diagnosing LDS and whether L4-L5 facet joint effusions predicted LDS.
Mr Kuhns emphasized that detecting LDS can have an impact on decision-making when preparing patients for lumbar surgery. Although the advantages of MRI include the ability to show canal stenosis and facet effusions that have been linked to LDS, Mr Kuhns emphasized that MRI often underestimates the severity of LDS and sometimes misses it altogether.
Mr Kuhns and colleagues retrospectively reviewed 103 patients with LDS. Patients were included in the study if they had a LDS defined radiographically as a slip > 4.5 mm. Mobile LDS was defined as a slip reduction > 3% between SLFE and MRI.
Two independent examiners reviewed other measurements, including the L4–L5 facet effusion diameter on axial MRIs. The kappa coefficient was used to assess the interobserver agreement with > 75 demonstrating excellent agreement.
The study found MRI-detected radiographic spondylolisthesis in 80 of 103 patients (78% sensitivity) vs 101 of 103 patients (98% sensitivity) with SLFE. The interobserver agreement was ≥ 0.8. MRI was associated with a significantly lower slip percentage than SLFE (19.8% vs 22.7%; P < .0001) and a higher anterior height (9.2 mm vs 8.4 mm; P <.0001).
When dividing the cohort of patients into mobile LDS and nonmobile LDS, the data suggest that 48% of the entire cohort had mobile LDS and that mobile LDS had a significantly greater x-ray slip percentage compared with nonmobile LDS (24.4% vs 21.2%; P =.02) and a smaller MRI slip percentage (17.4% vs 22.1%; P = .0007).
In addition, the patients with mobile LDS also had a larger mean effusion width than patients with nonmobile LDS (2.0 mm vs 1.2 mm; P =.0016) and a greater number of effusions > 2 mm (Table 1).
Results Comparing Mobile LDS With Nonmobile LDS
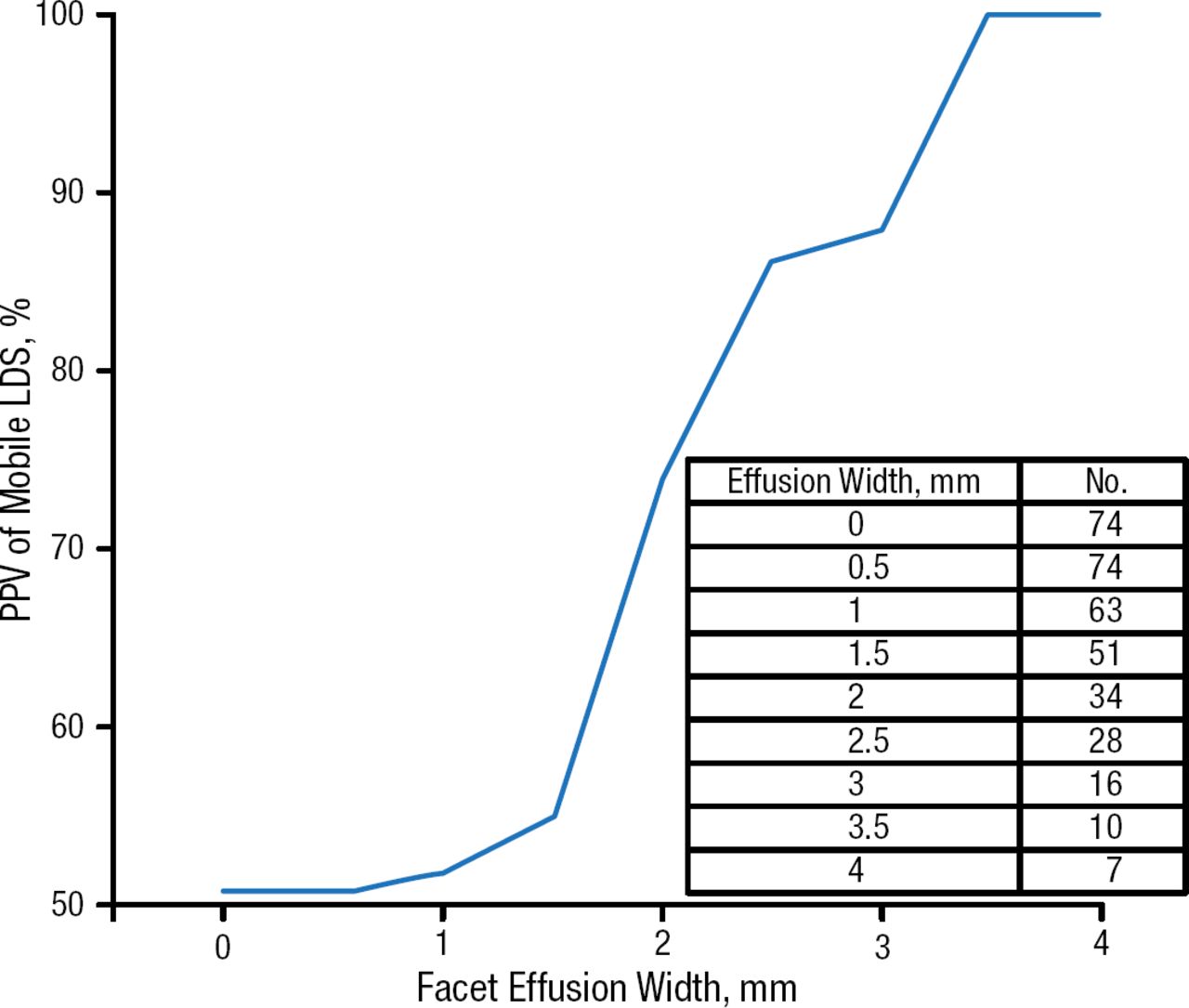
The study also looked at the positive predictive value (PPV) of effusions for mobile LDS and found that the PPV increased from around 50% for a 1 mm effusion to 86% for a 2.5 mm effusion. For effusions > 3.5 mm, the PPV increased to 100% (Figure 1).

PPV of Effusions for Mobile LDS
LDS, lumbar degenerative spondylolisthesis; PPV, positive predictive value.
Adapted from The Spine Journal, Kuhns BD et al, Sensitivity of magnetic resonance imaging in the diagnosis of mobile and nonmobile L4–L5 degenerative spondylolisthesis. Online Ahead of Print, In Press, Corrected Proof, doi: 10.1016/j.spinee.2014.08.006. Accessed 12/8/2014. Copyright (2014), with permission from Elsevier, Inc.
Mr Kuhns also highlighted key findings, including the lower sensitivity of MRI compared with SLFE to detect LDS (78% vs 98%) and the PPV of increasing facet effusion width to predict mobile L4–L5 LDS.
- © 2015 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.