

Summary
Tendinosis is a common health concern that may be resistant to treatment, making it important to consider the best approaches. This article reviews the options for treating tendinosis.
- interventional radiology
- ultrasonography
- orthopaedic procedures
- soft tissue disorders
Tendinosis is a common health concern that may be resistant to treatment, making it important to consider the best approaches. In this session, 3 presenters reviewed the options for treating tendinosis.
TENDON FENESTRATION FOR TENDINOSIS
Jon A. Jacobson, MD, University of Michigan Health System, Ann Arbor, Michigan, USA, reviewed the procedure and outcomes for tendon fenestration as a treatment for tendinosis, a condition in which there is degeneration and possible microtears in a tendon without inflammation. In tendinosis, the tendon is hypoechoic and swollen; it may have anechoic clefts with tears or hyperemia. Tendon fenestration is an approach in which a needle is passed through the affected areas to disrupt the tendinosis. It can cause bleeding, the release of growth factors, and stimulate healing.
At least 10 days prior to fenestration, it is important for patients to discontinue any nonsteroidal anti-inflammatory drugs (NSAIDs) to allow inflammation and healing to occur. However, Dr Jacobson does not recommend the discontinuation of aspirin for a cardiovascular event because of the trade-off of risks and benefits. Using ultrasound (US) guidance, a 20- to 22-gauge needle is passed through the tendon 20 to 30 times to cover the entire abnormality, pulling out the needle from the tendon (but not through the skin) when redirection is needed.
Contraindications have not been well defined, but some recommend caution with recent steroid injections (< 3 months prior), bleeding disorders, infections, or tendon tears that are > 50% of tendon thickness [Chiavaras MM, Jacobson JA. Semin Musculoskelet Radiol. 2013]. Following the procedure, Dr Jacobson recommends that patients rest; NSAIDs and ice should be avoided for 2 weeks. Some physicians recommend additional restrictions such as a knee brace.
Dr Jacobson then summarized the literature on fenestration and the associated techniques for tendinosis (Table 1). While the research is relatively limited, overall, most of the literature suggests improvement and that patients tolerate the procedure well. He noted that corticosteroids do not appear to help and interfere with inflammatory processes [McShane JM et al. J Ultrasound Med. 2008]. More data are needed concerning associated procedures such as platelet-rich plasma (PRP), whole blood injection, hyperosmolar dextrose, and prolotherapy. In the future, it will be important to learn more about which patients benefit, the appropriate timing, and the optimal number of treatments.
Summary of Studies on Tendon Fenestration
PRP FOR TENDINOSIS
Kenneth S. Lee, MD, University of Wisconsin School of Medicine and Public Health, Madison, Wisconsin, USA, addressed the associated treatment of PRP in more detail, including a review of the current literature and uses for PRP therapy. Although there can be variability in its preparation, PRP is defined in the literature as platelet count with 1 000 000 per μL.
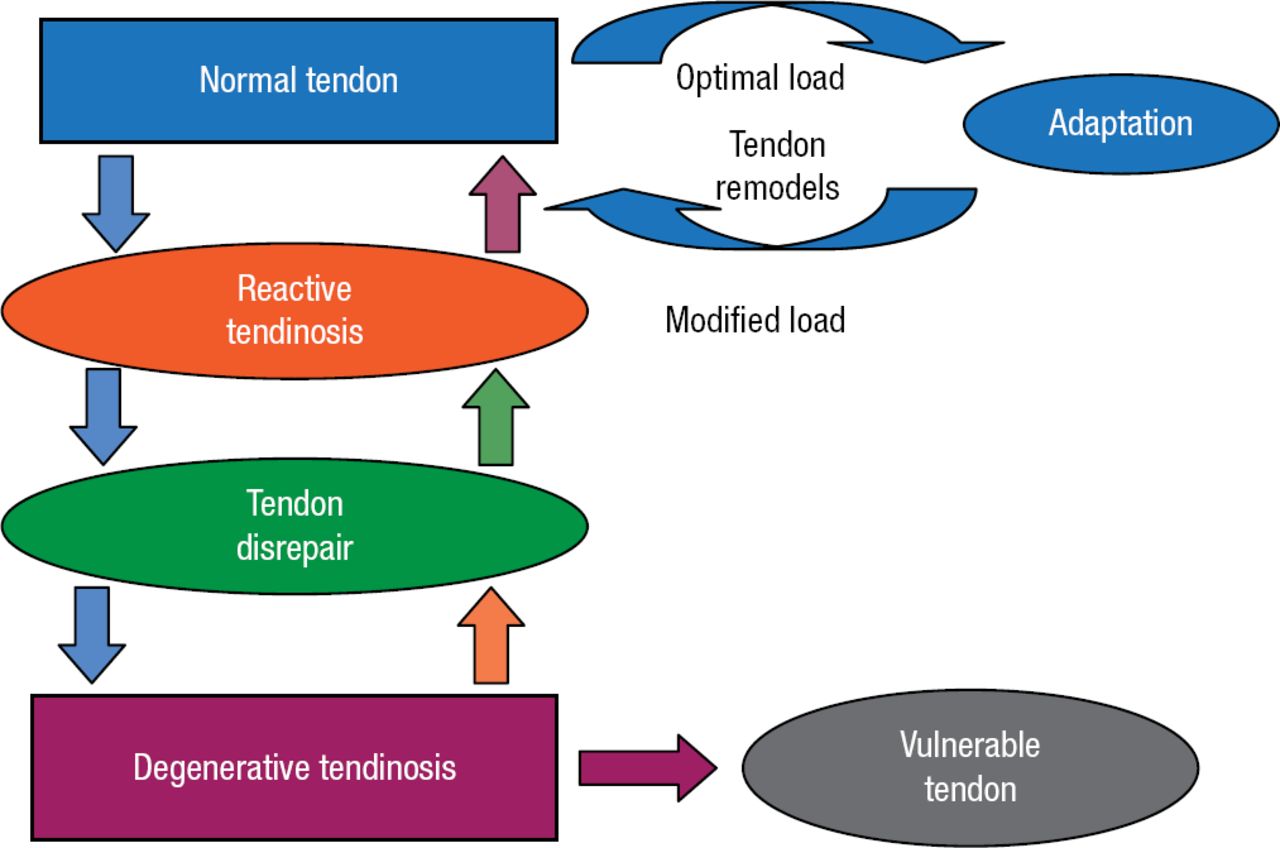
Tendinosis is a substantial, common health issue [Woodwell DA, Cherry DK. Adv Data. 2004] that can be difficult to treat; it is responsible for a high percentage of athletic injuries. The purpose of PRP therapy is to encourage healing and remodeling, which disrupts the progression of degenerative tendinosis (Figure 1). Although conservative management is sufficient to relieve pain and return function in about 80% of patients, healing takes time and the tendon remains vulnerable [Wilson JJ, Best TM. Am Fam Physician. 2005]. There is limited, inconsistent evidence about the best approaches for treatment.

Tendinosis Model
Reproduced with permission from KS Lee, MD.
Current US-guided therapies include steroids, percutaneous needle tenotomy (fenestration), prolotherapy, and PRP therapy. PRP therapy has become more common and is used for lateral epicondylitis, patellar tendinosis, and plantar fasciopathy, among others. The benefits arise from the interplay of concentrated growth factors (eg, platelet-derived growth factor, transforming growth factor-β, and basic fibroblast growth factor) in a relatively hypovascular area.
PRP is recommended for chronic overuse injuries, injuries that do not respond to conservative therapy, cases in which surgery is unwanted or inappropriate, and for accelerating return to play for athletes with acute injuries. There is generally a single injection followed by immobilization for 24 to 72 hours and then a gradual increase in activity after a month. Although the procedure is safe, pain medication may be required following injection. NSAIDs should be avoided as they interfere with healing. Although one study indicated that PRP was significantly more effective (P < .001) than steroid treatment [Peerbooms JC et al. Am J Sports Med. 2010], another study did not find PRP to be more effective than saline after 1 year [de Vos RJ et al. JAMA. 2010]. Preliminary data from a pilot randomized controlled trial of 44 patients with plantar fasciopathy suggested significantly greater improvements in visual analog score for pain in patients treated with PRP vs steroids (P < .001).
Dr Lee concluded by emphasizing the importance of studying tendinosis due to the prevalence of the problem, and the markedly increasing use of PRP despite larger randomized controlled trials. A standard of care needs to be established.
OTHER TREATMENTS FOR TENDINOSIS
Concluding the session, Mary M. Chiavaras, MD, PhD, McMaster University, Hamilton, Ontario, Canada, presented an overview of treatments for tendinosis. She first reviewed the IMPROVE randomized controlled trial [Chiavaras MM et al. Acad Radiol. 2014] that is comparing PRP, whole blood, fenestration, and physical therapy. Factors influencing the best approach for a particular patient include the type of pathology, goals of the patient, type of patient (eg, athlete or nonathlete), and legality.
Treatments can be noninvasive, percutaneous minimally invasive, or surgical. Noninvasive treatments are commonly used and can be effective in many cases. For the acute phase, it is important to modify risk factors (eg, stop the injury). Many patients try to minimize inflammation, but inflammation is important in healing. In the chronic phase, healing has failed and degeneration has occurred; NSAIDs are not helpful. The most common intervention is eccentric exercise [Frizziero A et al. Br Med Bull. 2014], which may promote remodeling and collagen cross-link formation while decreasing pain mediators [Maffulli N et al. J Bone Joint Surg Am. 2010]. Some other noninvasive interventions include deep-friction tissue massage, low-intensity laser therapy, therapeutic ultrasonography, and extracorporal shockwave therapy.
Percutaneous minimally invasive procedures include a wide range of possibilities, such as PRP and fenestration; some illegal approaches have been tried (eg, deer antler dust). Corticosteroids have risks such as increased risk of tendon rupture, fat atrophy, depigmentation, and elevated glucose levels [Moon HJ et al. Am J Phys Med Rehabil. 2014; McMahon SE et al. Acta Orthop Belg. 2013]. Corticosteroids should not be injected into tendons.
Prolotherapy involves the injection of an irritant, such as hyperosmolar dextrose, which may cause an inflammatory response, the release of growth factors, and healing [Rabago D et al. Am J Phys Med Rehabil. 2013; Distel LM, Best TM. PM R. 2010]. Finally, ultrasonic percutaneous tenotomy is a new treatment that involves a US Food and Drug Administration–approved device that is used to remove pathological tissue and that produced improvements in one study [Barnes DE et al. J Shoulder Elbow Surg. 2015].
Prof Chiavaras concluded by highlighting the importance of trying physical therapy first, using caution with steroids, and considering fenestration if physical therapy was not sufficient.
- © 2015 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.