

Summary
This article reviews existing noninvasive technologies in dermatology, including imaging and nonimaging tools. The speakers presented data on these technologies and discussed their clinical applicability, as well as new technology concepts from preclinical research.
- Skin Cancer
- Soft Tissue Cancers
- Dermatology
- Skin Cancer
- Soft Tissue Cancers
This session reviewed existing noninvasive technologies in dermatology, including imaging and nonimaging tools. The speakers presented data on these technologies and discussed their clinical applicability, as well as new technology concepts from preclinical research.
MORE EVIDENCE NEEDED ON QUALITY AND CONSISTENCY OF NONINVASIVE DIAGNOSTIC TOOLS
The diagnosis of melanoma by simple visual examination using the ABCD method is incorrect in almost 1 of every 3 invasive melanoma diagnoses. A number of new techniques have improved the noninvasive diagnosis of slow-growing superficial spreading melanoma. Early diagnosis of fast-growing nodular melanoma may not be possible (or practical), however, using these costly diagnostic technologies. Josep Malvehy, MD, Hospital Clinic of Barcelona, Barcelona, Spain, reviewed the utility of available noninvasive methods for early melanoma diagnosis.
Qualitative imaging methods for melanoma diagnosis include dermoscopy, total body photography, multiphoton tomography, reflectance confocal microscopy (RCM), and optical coherence tomography (OCT). Quantitative methods using automated analysis include multispectral imaging, electrical impedance spectroscopy, and Raman spectroscopy. The features and key study results of the first 3 qualitative methods and the first 3 quantitative methods are shown in Table 1. RCM and OCT were discussed in the subsequent presentations.
Noninvasive Qualitative and Quantitative Methods for Melanoma Diagnosis
A study of a new noninvasive adhesive patch test for evaluation of pigmented lesions using a 2-gene (CMIP and LINC00518) signature assay for differentiating melanomas from pigmented lesions reported a sensitivity of 97.6% and specificity of 72.7% [Gerami P et al. J Am Acad Dermatol. 2014]. Limitations of this study included the loss of cases due to messenger RNA insufficiency, inclusion of limited melanoma subtypes, and a minimum lesion diameter of 4 mm.
Prof Malvehy concluded that new technologies for noninvasive detection of skin cancer will be developed and others will disappear. The optimal method for diagnosis depends on the physician, patient population, technical issues, and stage of development. Important questions remain about the clinical benefit, cost, and evidence for quality and consistency of noninvasive tools for diagnosing skin cancer.
NEAR HISTOLOGIC RESOLUTION OF MELANOMA WITH RCM
Giovanni Pellacani, MD, University of Modena, Modena, Italy, spoke about in vivo imaging of the skin with RCM in clinical practice and research. RCM provides lateral resolution of 0.5 to 1 μm and axial resolution of 3 to 4 μm. The technique is noninvasive and painless, and it takes 7 minutes to acquire an image, providing an optical biopsy with cellular resolution. The confocal technology produces a composite grayscale image that is formed by consecutive confocal frames and mounted together to form a horizontal section of an area up to 8 × 8 mm to a maximum depth of 300 μm.
Melanoma is diagnosed on an RCM image by looking for the same features observed on histopathology, including large round pagetoid cells and nonhomogeneous junctional nests of atypical cells. Nevi, on the other hand, are characterized by a ringed, meshwork, or clod pattern without the large atypical cells seen in melanoma.
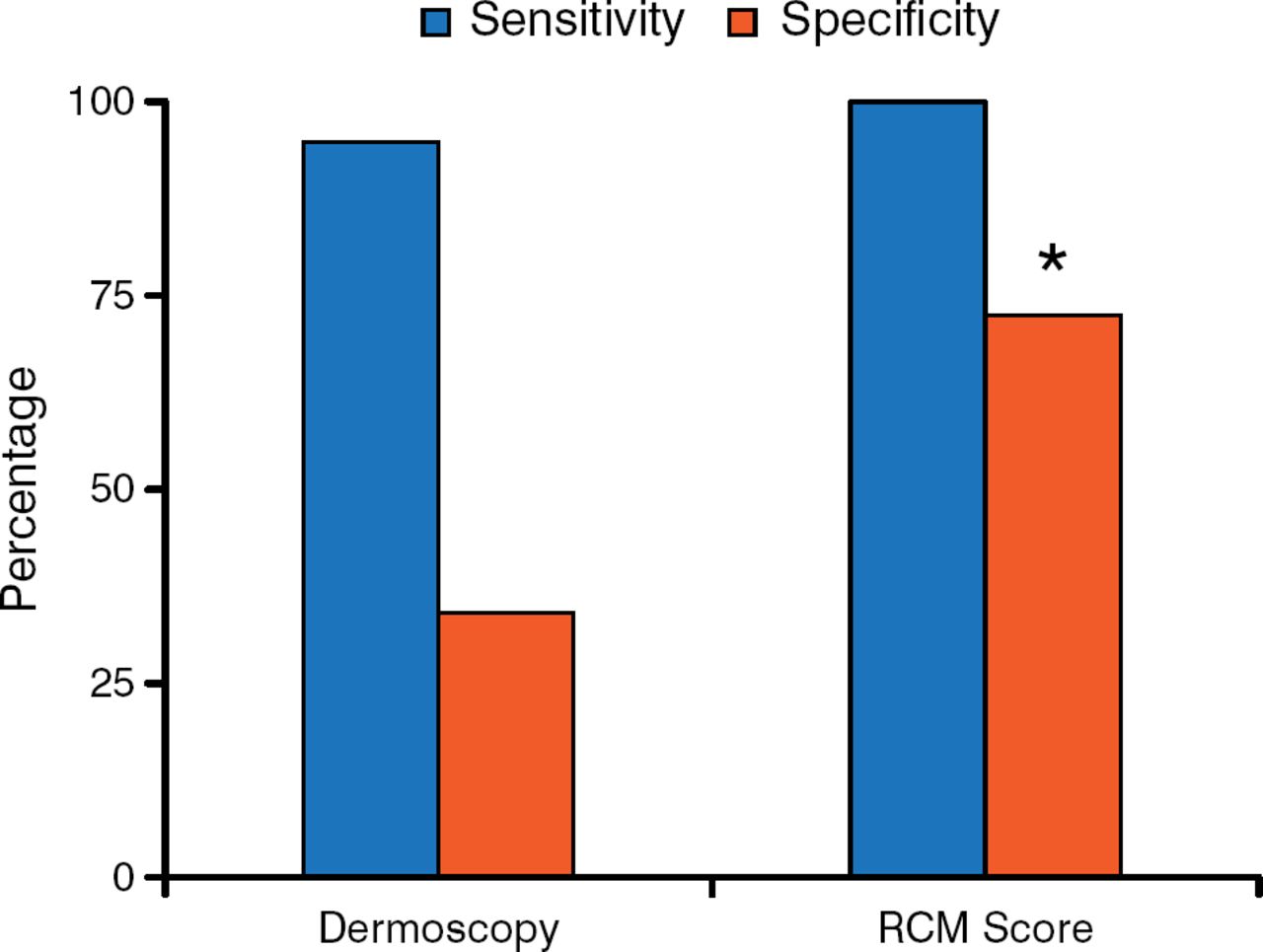
Guitera and colleagues [J Invest Dermatol. 2009] demonstrated superior specificity with RCM (68%; 95% CI, 61.1% to 74.3%) vs dermoscopy (32%; 95% CI, 25.9% to 38.7%) and similar sensitivity with RCM (91%; 95% CI, 84.6% to 95.5%) and dermoscopy (88%; 95% CI, 80.7% to 92.6%) in the secondary evaluation of melanocytic lesions (Figure 1).

Sensitivity and Specificity of Reflectance Ccnfocal Microscopy vs Dermoscopy in Secondary Evaluation of Melanocytic Lesions
RCM, reflectance confocal microscopy.
*P < .001.
Data source: Guitera P et al. J Invest Dermatol. 2009.
Reproduced with permission from G Pellacani, MD.
An analysis of 710 consecutive clinically equivocal lesions found that RCM had 87.6% sensitivity and 70.8% specificity for melanoma [Guitera P et al. J Invest Dermatol. 2012].
A 10-year study of the accuracy of melanoma detection found that the number needed to excise a melanoma was 8.7 in specialized centers and 29.4 in nonspecialized centers [Argenziano G et al. J Am Acad Dermatol. 2011]. Pellacani and colleagues [Br J Dermatol. 2014] recently reported that the number needed to excise a melanoma with RCM examination at a melanoma clinic was 6.8.
A study correlating melanoma biomarker levels with RCM found that melanomas with higher Bak serum levels had more junctional activity on RCM, whereas those with weak Bak expression had sparse dermal nests on RCM [Longo C et al. Exp Dermatol. 2011]. Another study reported that distinct melanoma subtypes were identified by RCM analysis of cell morphology [Pellacani G et al. Exp Dermatol. 2014]. Furthermore, melanoma risk identification and early diagnosis were improved with both RCM and dermoscopy when combined with genetic studies [Bassoli S et al. Exp Dermatol. 2013].
RCM analyzes skin lesions in vivo with similar resolution as observed with histology. According to Prof Pellacani, in vivo morphology may represent the missing link to bridge clinical and laboratory research.
OCT IMPROVES DIAGNOSTIC ACCURACY AND SPECIFICITY IN NONMELANOMA SKIN CANCER
Martina Ulrich, MD, Collegium Medicum Berlin, Berlin, Germany, discussed the use of OCT for diagnosing nonmelanoma skin cancer. OCT provides up to 60 images per scan of vertical and horizontal skin sections with a resolution of 7.5 μm up to 2 mm deep. High-resolution OCT combines horizontal and vertical imaging and has a 1.6 × 1.8 mm imaging field, 3 μm resolution, and 570 μm penetration. Multibeam OCT also combines horizontal and vertical imaging, and it has a 6 × 6 mm imaging field, 7.5 μm resolution, and 1 to 2 mm penetration.
OCT is used for differentiating nonmelanoma skin cancers from benign lesions, defining tumor thickness, and assessing tumor margins. A study of basal cell carcinoma diagnosis with OCT vs clinical evaluation and dermoscopy in 235 lesions demonstrated a diagnostic accuracy of 65.8% for histology, 76.2% for dermoscopy, and 87.4% for OCT. The positive predictive value and negative predictive value were greatest with OCT.
In the same study, OCT significantly improved specificity vs clinical and vs dermoscopy (P < .0001 for both) but not sensitivity vs clinical evaluation (P = .099) and dermoscopy (P = .121). Table 2 shows the results of additional studies of OCT for the diagnosis and evaluation of nonmelanoma skin cancers.
Studies of OCT for Diagnosis of Nonmelanoma Skin Cancer
OCT is applicable for the primary diagnosis of non-melanoma skin cancer. It may prove to be a useful tool for determining vertical tumor thickness. OCT also allows monitoring of lesions throughout time, and improves the diagnostic accuracy when evaluating pink patches. OCT increases diagnostic specificity in equivocal lesions compared with dermoscopy and clinical examination.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.