

Summary
Vaginal hysterectomy (VH) is the most minimally invasive approach for hysterectomy in women with benign gynecologic disease. During the Donald F. Richardson Memorial Lecture, Rosann M. Kho, MD, formerly of the Mayo Clinic, Scottsdale, Arizona, USA, stated that it is time to transform the view of VH to increase its use and provide benefit to more women, most of whom would qualify for this approach. This requires defining new patient selection criteria while incorporating new surgical technologies, devices, and techniques to overcome the traditional challenges that have limited the use of VH.
- Diagnostic & Surgical Procedures
- Diagnostic & Surgical Procedures
- Obstetrics & Gynecology
Vaginal hysterectomy (VH) is the most minimally invasive approach for hysterectomy in women with benign gynecologic disease. In the Donald F. Richardson Memorial Lecture, Rosann M. Kho, MD, formerly of the Mayo Clinic, Scottsdale, Arizona, USA, stated that it is time to transform the view of VH to increase its use and provide benefit to more women, most of whom would qualify for this approach. This requires defining new patient selection criteria while incorporating new surgical technologies, devices, and techniques to overcome the traditional challenges that have limited the use of VH.
The current evidence demonstrates that VH, compared with the other approaches, is associated with improved outcomes and fewer complications, according to a statement from the American College of Obstetrics and Gynecology [ACOG Committee. Obstet Gynecol 2009].
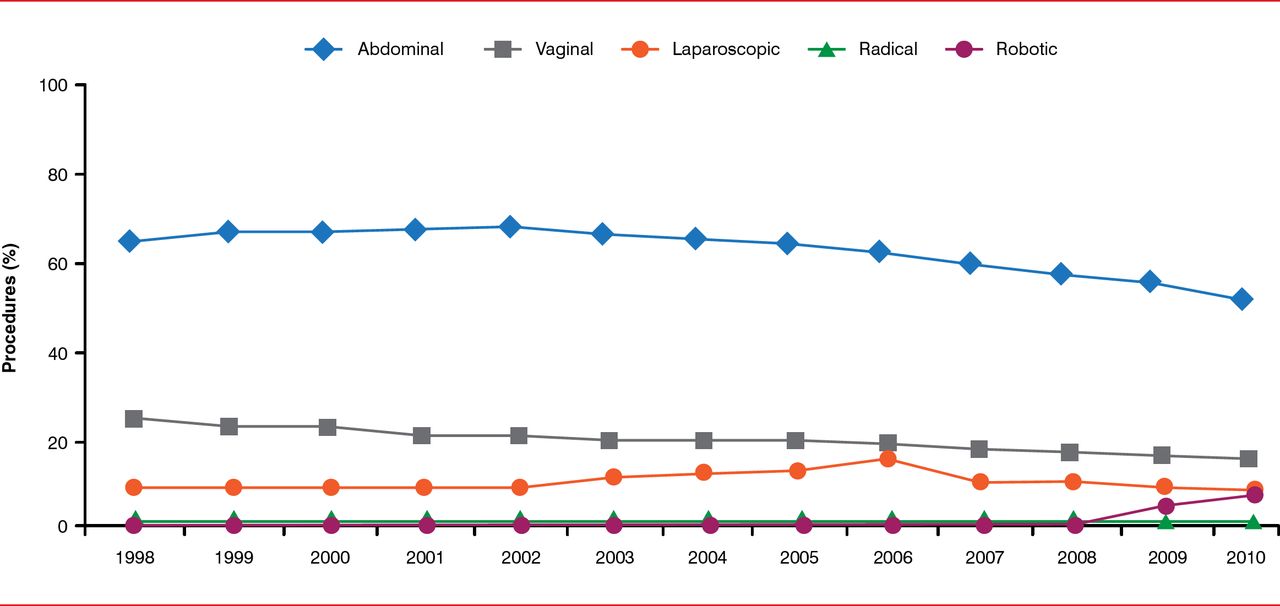
Yet, the national rates of inpatient hysterectomy are declining, including a significant decline in VH, from >25% of all hysterectomies in 2000 to <17% in 2010 (Figure 1) [Wright JD et al Obstet Gynecol 2013]. Furthermore, surgeon volume is decreasing, with >80% of surgeons performing <5 VH annually and <5% performing >10 VH annually [Rogo-Gupta LJ et al. Obstet Gynecol 2010]. Data from Wright and colleagues [JAMA 2013] showed that from 2007 through 2010 the rates of abdominal hysterectomy declined by 14% and VH by 2%, while rates of laparoscopic hysterectomy decreased by 6% and robotically assisted hysterectomy increased by 9.5%. This shift in approach to hysterectomy is associated with increased cost. One institution reported in 2009 that when compared to the vaginal approach, abdominal, laparoscopic, and robotic approaches cost $12 000 to $18 000 more per patient [Wright KN et al. JSLS 2012].

Rates of Hysterectomy in the United States by Surgical Approach, 1998 Through 2010
Reproduced from Wright JD et al. Nationwide trends in the performance of inpatient hysterectomy in the United States. Obstet Gynecol. 2013;122(2, pt 1):233–241. With permission from Lippincott, Williams and Wilkins.
Experience in performing VH during residency is also decreasing, from 35 cases in 2002 to 19 cases in 2012 per resident over 4 years [Washburn EE. J Minim Invasive Gynecol 2013]. Dr. Kho called this a national health care crisis, with ob-gyn residents insufficiently trained to provide the benefit of this preferred minimally invasive surgical approach, which in turn increases the burden on the health care system.
ADDRESSING TECHNICAL CHALLENGES IN VH
According to Dr. Kho, multiple studies in the literature have demonstrated that the traditional challenges for VH can be addressed. Lessons learned from the laparoscopic and robotic approaches can be applied to address these technical challenges in the vaginal approach. Common challenges have been poor exposure (including previous pelvic surgery), inadequate hemostasis, difficult entry into the anterior cul-de-sac, large uterus (>12 weeks), poor vaginal descent or no prior vaginal delivery, avoiding bladder and ureteral injury, and removal of ovaries or fallopian tubes. She proposed that these surgical environments are often used as reasons to avoid performing VH and excuses for achieving inadequate training.
Dr. Kho notes that exclusion criteria for VH are pain (other than menses related) and suspicion of cancer. Patients with infiltrating endometriosis benefit from a laparoscopic or robotic approach to hysterectomy. Morcellation through any route, including a minimally invasive approach, should not be performed in patients with a high index of suspicion of cancer.
A first step in addressing the technical challenges is improving ergonomics for the surgeon and the entire team. Dr. Kho recommends ensuring that the chairs for the surgeon and assistant be at eye level of the operating field, with shoulders in a comfortable position and elbows at the side, and that a footstool be used as needed for stabilization. A magnetic pad is useful to hold surgical tools at hand. A monitor facilitates the procedure and education by permitting the entire surgical team to view the procedure. Recording the procedure for education via headgear with an attached camera is also recommended.
Dr. Kho advises that the surgeon deconstruct the procedure to anticipate all possible difficulties and to have the necessary equipment and devices available. Approaches to improve exposure include use of the Magrina-Bookwalter vaginal retractor, fiberoptic light, Mayo modified long and extra-long Deaver retractors, long instruments, and a single long pack to keep the bowel away.
Routine intraoperative cystoscopy should be used during hysterectomy, regardless of the approach, because multiple studies have shown that intraoperative injury to the bladder and ureters can be diagnosed before the patient leaves the operating room.
Entry into the anterior cul-de-sac is facilitated by delaying it until better descensus is achieved, by sharply lysing bladder adhesions, sealing and dividing the uterine arteries and cardinal ligaments, and starting morcellation. Regarding the challenge of the large uterus, Dr. Kho stated that the principles remain the same for a 12-week-sized uterus, as with any larger uterus. This includes use of morcellation, only after the uterine arteries are ligated, by bivalving the cervix and performing a wedge excision with a long curved knife. Avoidance of digging into an area that is not well visualized and having adequate light can also aid with larger uteri. Many tools have been modified with a light to improve visualization, but she noted that the tools can be hot; thus, caution should be used to avoid leaning them against the vaginal wall.
Dr. Kho indicated the signs that the vaginal procedure should be converted to a minilaparotomy or laparoscopic approach to complete the hysterectomy: excessive bleeding, inability to bilaterally secure uterine arteries, a portion of loose bowel that obscures the surgeon's view, excessive debris from morcellation, or a large anterior fibroid that will not move down into the pelvic canal.
Prophylactic salpingectomy can be performed vaginally for women with BRCA1 or BRCA2 gene mutations that increase their risk of ovarian cancer. In November 2013, the Society of Gynecological Oncology released a statement on the use of salpingectomy in this regard [SGO Statement 2013], because of increasing evidence that the fallopian tubes may be the source of pelvic serous carcinomas.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.