

Summary
Soybean oil lipid emulsions for parenteral nutrition have been used since the 1960s. Alternative oils were developed to reduce the phytosterols and linoleic acid in soybean oil emulsions, which promote the stress response, suppress immune function, and impair liver function. Clinical studies have demonstrated that olive and other oil sources are safe and effective in adult and pediatric patient populations.
- lipid
- emulsion
- parenteral
- nutrition
- pediatric
- adult
- soybean
- olive
- fish
- inflammation
- stress
- immune
Intravenous fat emulsions (IVFEs) based on soybean oil have been the standard for parenteral nutrition (PN) for over 50 years. Although alternative IVFEs have been available for some time, US practitioners have only recently gained access to these products. Kathleen M. Gura, PharmD, Boston Children’s Hospital, Boston, Massachusetts, USA, described the content and benefits of these IVFEs and the limitations associated with soybean oil monotherapy.
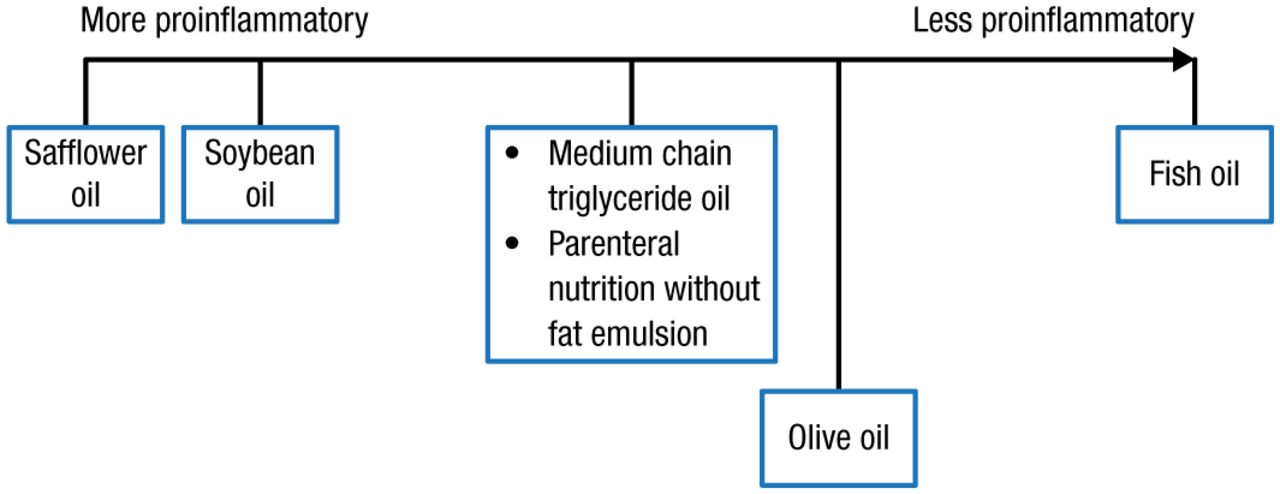
IVFEs provide essential fatty acids (EFAs) for PN and are an alternative source of nonprotein calories. EFAs function in cellular proliferation and maintenance of cell membrane structure. While omega-5, omega-7, and omega-9 lipids are synthesized in the body, the omega-3 and omega-6 EFAs must be obtained from exogenous sources. Soybean oil is composed of 50% linoleic acid (omega-6), 25% oleic acid (omega-9), and 10% alpha-linolenic acid (omega-3) [Vanek VW et al. Nutr Clin Pract. 2012]. Soybean oil is also rich in phytosterols and is considered to be more proinflammatory than medium-chain triglycerides (MCTs), olive oil, and fish oil (Figure 1). Soybean oil IVFEs provide excessive linoleic acid, altering cell membrane structure and increasing eicosanoid production, resulting in increased inflammation and decreased cell-mediated immunity [Waitzberg DL et al. JPEN J Parenter Enteral Nutr. 2006].
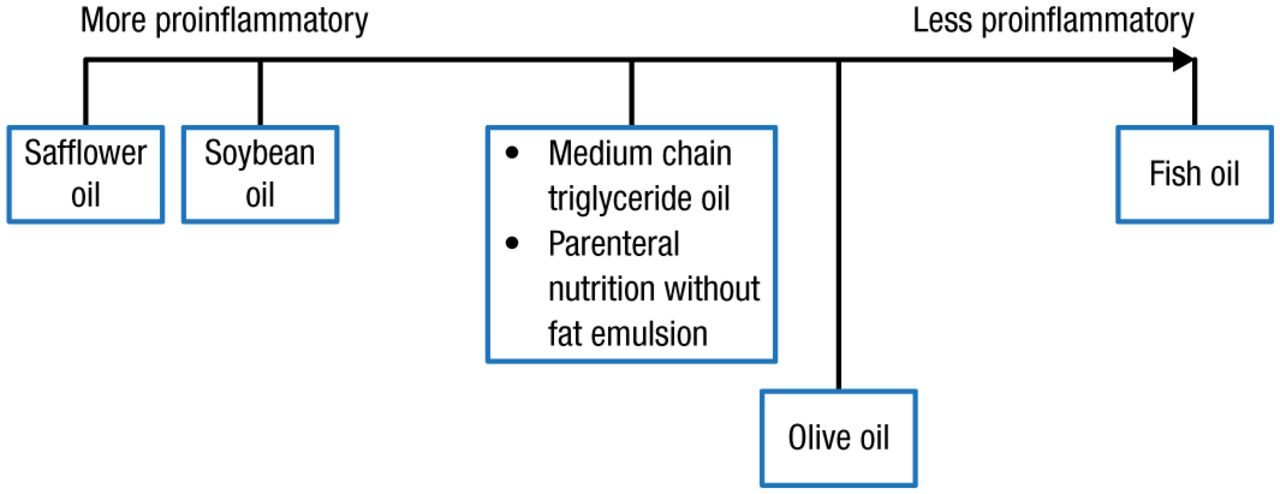
Inflammatory Characteristics of Oils Used in IVFEs
IVFE, intravenous fat emulsion.
Adapted from Vanek VW et al. Nutr Clin Pract. 2012;27(2):150-192. Copyright © 2012 by American Society for Parenteral and Enteral Nutrition. Reprinted by Permission of SAGE Publications.
Newer IVFEs were developed to reduce the linoleic acid load in PN [Waitzberg DL et al. JPEN J Parenter Enteral Nutr. 2006]. These products include various combinations of soybean oil, MCTs, olive oil, and fish oil, which differ in phytosterol content, vitamin E content, and inflammatory characteristics. IV phytosterols, such as those present in soybean oil IVFEs, are metabolized in the liver and may contribute to liver injury, especially in neonates in whom phytosterols accumulate [Pianese P et al. J Pediatr Gastroenterol Nutr. 2008]. The phytosterol content in IVFE products reflects the amount of soybean oil present. Vitamin E concentrations are highest in fish and mixed oil products and are low in soybean oil IVFEs. Vitamin E prevents hepatic injury in animal models and may be lower in plasma lipoproteins with prolonged use of soybean oil IVFEs.
IVFEs have been approved for use in the United States based on their ability to provide calories and EFAs. Their efficacy and safety are difficult to compare because many IVFE trials to date have been underpowered to show statistically significant changes in clinical outcomes. The Canadian Clinical Evaluation Research Unit’s critical care nutrition recommendations suggest withholding IVFEs high in soybean oil in critically ill, well-nourished patients but state that data are insufficient to recommend withholding IVFEs high in soybean oil in malnourished critically ill patients or those requiring prolonged courses of PN > 10 days [Canadian Clinical Practice Guidelines. 2013]. The American Society for Parenteral and Enteral Nutrition has concluded that alternative oil-based IVFEs are safe and effective alternatives to soybean oil IVFEs [Vanek VW et al. Nutr Clin Pract. 2012].
Soybean oil IVFEs increase the inflammatory response and suppress cell-mediated immune function in severely stressed surgical patients [Furukawa K et al. Nutrition. 2002] and T-cell and natural killer cell function, increasing susceptibility to infection in trauma patients according to a 1997 study [Battistella et al. J Trauma. 1997]. Reports like these led to the development of IVFEs with a reduced concentration of linoleic acid. Philip Calder, PhD, University of Southampton, Southampton, United Kingdom, discussed alternatives to soybean oil in IVFEs, particularly olive oil.
Olive oil is rich in oleic acid and low in linoleic acid. It contains vitamin E and other antioxidants and is generally considered a healthy oil. An IVFE consisting of an 80:20 mix of olive and soybean oils was introduced in the 1990s. It contains 64% oleic acid, 20% linoleic acid, 12% palmitic acid, and 2% each of alpha-linolenic and stearic acid. Olive oil IVFE is now preferred and is in routine use in many institutions in Europe, Asia, Australia, and New Zealand. The olive-soybean oil blend is safe and may improve liver function, oxidative stress, and immune function when compared with soybean IVFEs [Sala-Vila A et al. Curr Opin Clin Nutr Metab Care. 2007].
Olive-soybean oil IVFE has been studied for home PN in children and adults, in preterm and critically ill infants, and in critically ill and postsurgical adults. In a 1999 study, in children receiving home PN, no difference was observed in plasma lipids or liver function enzymes, but lipoprotein peroxidation was lower with olive-soybean oil versus soybean oil IVFE. Studies in preterm and critically ill infants reported similar plasma lipids, liver function enzymes, immune function, and oxidative stress markers; higher vitamin E; and lower interleukin-6 production with olive versus soybean oil emulsion [Demirel G et al. Early Hum Dev. 2012; Roggero P et al. Nutrition. 2010; Deshpande GC et al. J Pediatr Gastroenterol Nutr. 2009; Hartman C et al. Clin Nutr. 2009; Gawecka A et al. JPEN J Parenter Enteral Nutr. 2008; Gobel Y et al. J Pediatr Gastroenterol Nutr. 2003].
Table 1 summarizes results of studies comparing olive-soybean and soybean oil IVFEs in adults.
Studies Comparing Olive-Soybean With Soybean Lipid Emulsions in Adults
A prospective multicenter study compared the effects of lipid-free PN (n = 70) or PN involving soybean oil (n = 223), MCTs (n = 65), olive oil (n = 73), or fish oil (n = 19) IVFEs on clinical outcomes in 451 critically ill ventilated patients admitted to the intensive care unit (ICU) [Edmunds CE et al. Crit Care Med. 2014]. The secondary analysis end points were time to termination of mechanical ventilation alive, time to ICU discharge alive, and time to hospital discharge alive. Clinical outcomes for all the groups at 60 days after ICU admission are shown in Table 2.
Clinical Outcomes at 60 d Following ICU Admission
When compared with those who received soybean oil, patients who received olive oil had a shorter time to termination of mechanical ventilation alive (HR, 1.43; 95% CI, 1.06 to 1.93; P = .021) and a shorter time to ICU discharge alive (HR, 1.76; 95% CI, 1.30 to 2.39; P < .001). The time to hospital discharge alive was not significantly different than that in the other groups (HR, 1.25; 95% CI, 0.89 to 1.75; P = .199).
Olive-soybean oil lipid emulsion for PN appears to be safe in children and adults. Little difference has been observed in most laboratory and clinical outcomes between olive and soybean oil IVFEs. Fatty acid profiles are different with the 2 formulations, and in some studies vitamin E levels are higher with olive oil IVFE. Recent data from an international study found genuine benefits with the use of olive-soybean oil in critically ill patients [Gultekin G et al. Pak J Med Sci. 2014].
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.