

Summary
This article highlights select advances in the management of stroke, including stem cell therapy, endovascular therapy, and physical therapy. It discusses the gender and sex effect, the global importance of intracerebral hemorrhage, the role of the extracellular matrix in cerebral small vessel disease, and the clinical trials network, StrokeNet.
- StrokeNet
- Multi-PART
- RIGHT-2
- stem cell therapy
- endovascular therapy
- cerebral small vessel disease
- intracerebral hemorrhage
- microinfarcts
- physical therapy
In a plenary session, speakers shared highlights of recent advances and future directions in stroke management.
Joseph Broderick, MD, University of Cincinnati, Cincinnati, Ohio, USA, launched the session with an introduction of StrokeNet, the National Institute of Neurological Disorders and Stroke (NINDS) clinical trials network. Funded by the National Institutes of Health (NIH), this national network comprises multisite, phase 1 to phase 3 clinical trials in stroke prevention, acute treatment, and recovery.
Currently, 25 regional stroke centers and 255 hospitals are involved, and the network comprises a centralized infrastructure for administrative needs, including managing data and running trials. Protocols for trials can originate from within or outside the network, and industry involvement is also encouraged. Trial proposals are formally submitted to NINDS, and following a feasibility assessment by StrokeNet, they are ultimately subjected to NIH review and approval.
Dr Broderick explained that while clinical trial proposals can be exploratory or confirmatory, their fundamental reasoning must address one or more of the following:
-
An unmet medical need
-
A plausible biological mechanism
-
Preclinical data
-
Early clinical data
Large trials will likely exceed the capabilities of regional centers, and will therefore also utilize nonaffiliated hospitals, as well as non-US national networks involved in global trials.
Education also plays a critical role in StrokeNet; the program has an educational core and provides funding for fellows at each center, in addition to educational programs for fellows, coordinators, and physicians within the network. Education and training are also provided for each trial.
Although StrokeNet is in its early stages, Dr Broderick noted that several initial trials are already being implemented, and others are awaiting review.
Patricia D. Hurn, PhD, University of Texas, Austin, Texas, USA, urged physicians to consider sex and gender in the context of stroke. Discussing how stroke affects men and women differently, she emphasized that, in the US, stroke is more likely to occur in women who are older than men, less healthy, and living alone. After an episode of stroke, women are also more likely than men to be institutionalized, have a poor recovery, and have a worse quality of life.
She discussed connectivity differences between the male and female brain that have implications for where stroke occurs, and shared data from studies showing that every cell has a sex, as demonstrated, for example, by differences in how brain cells from male and female animals react to ischemic damage (Figure 1) [Liu M et al. J Cereb Blood Flow Metab. 2007].

Sex-Related Differences in How Brain Cells React to Ischemia
*P < .05.
Adapted by permission from Macmillan Publishers Ltd: J Cerebr Blood F Met. Liu M et al. Role of P450 aromatase in sex-specific astrocytic cell death. 2007;27:135–141. Copyright 2007.
Consequently, she stressed that future clinical trials must include both sexes, and noted that new NIH policy will likely also require consideration of sex differences in preclinical cell and animal studies [Clayton JA, Collins FS. Nature. 2014].
Considering the development of therapeutic interventions for stroke, Philip M. Bath, MD, University of Nottingham, Nottingham, United Kingdom, highlighted the need to move to a bidirectional model that involves repeating earlier clinical and preclinical animal stages to provide new information, strengthen existing evidence, and explain earlier findings in order to refine phase 3 technologies.
To this end, he described the need for multicenter preclinical studies. Similar to clinical studies, these trials involve numerous recruiting sites, are run by a steering committee, and are supported by a data-monitoring committee [Bath PMW et al. Int J Stroke. 2009].
The Multicentre Preclinical Animal Research Team (Multi-PART) project is an example of this approach. This collaborative effort in preclinical stroke studies will involve a beta test that will run in parallel with the RIGHT-2 trial, a follow-up to the recent, single-site RIGHT trial [Ankolekar S et al. Stroke. 2013]. According to Prof Bath, this will aim to confirm the importance of forward and backward translation, demonstrate the use of multicenter preclinical animal studies and multisite paramedic-led ambulance-delivered trials, and potentially lead to the development of new treatments for stroke in humans.
Gary K. Steinberg, MD, PhD, Stanford University, Stanford, California, USA, discussed the use of stem cell therapy for stroke. According to Dr Steinberg, bone marrow transplantation is now used to treat and cure some cancers, and intracoronary administration of bone marrow stem cells has recently also shown benefit in patients following acute and chronic myocardial infarction [Tian T et al. Atherosclerosis. 2014; Delewi R et al. Heart. 2013; Clifford DM et al. Cochrane Database Syst Rev. 2012]. Although currently there is no treatment to restore lost brain function following stroke, Dr Steinberg discussed data from studies that suggest stem cell therapy will have a role to play in the future therapy of stroke [Rosado-de-Castro PH et al. Stem Cells Dev. 2013; Bliss T et al. Stroke. 2007]. He explained that transplanted stem cells from various sources, including bone marrow and neural tissue, are thought to produce trophic factors that enhance endogenous brain repair mechanisms and modulate inflammation.
Although many questions about the use of stem cell transplantation in stroke therapy remain unanswered, Dr Steinberg noted that initial clinical studies suggest its feasibility, safety, and possible efficacy. This technology therefore holds great promise for stroke therapy, and at least 29 trials in this area are pending.
Although Colin P. Derdeyn, MD, Washington University, St. Louis, Missouri, USA, acknowledged the current achievements in endovascular therapy, he discussed the potential for better, faster revascularization, with prevention of secondary and reperfusion injury and enhanced patient recovery. In particular, he highlighted diagnostic technologies such as C-arm computed tomography angiography and perfusion imaging that enable patients to be triaged in the interventional suite. In addition, the use of larger and more deliverable suction catheters, as well as capture devices such as the next-generation stent-retriever devices that are in development, can improve revascularization.
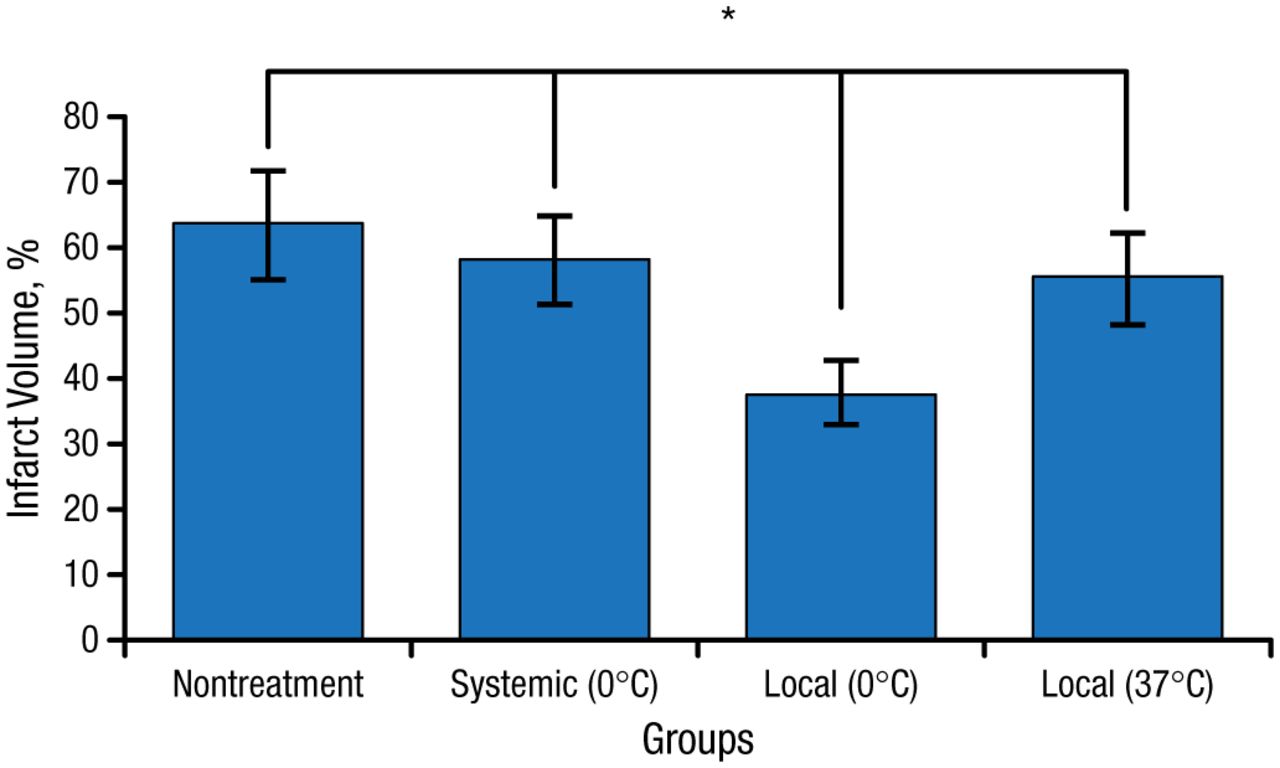
Dr Derdeyn also discussed the importance of neuroprotection and the prevention of secondary reperfusion injury, sharing data from a rodent cerebral ischemia study in which a microcatheter was used to occlude the middle cerebral artery [Chen J et al. Neurol Res. 2015]. In this study, infarct volumes were much smaller in animals when cold saline was injected into the brain just prior to removing the microcatheter (Figure 2).
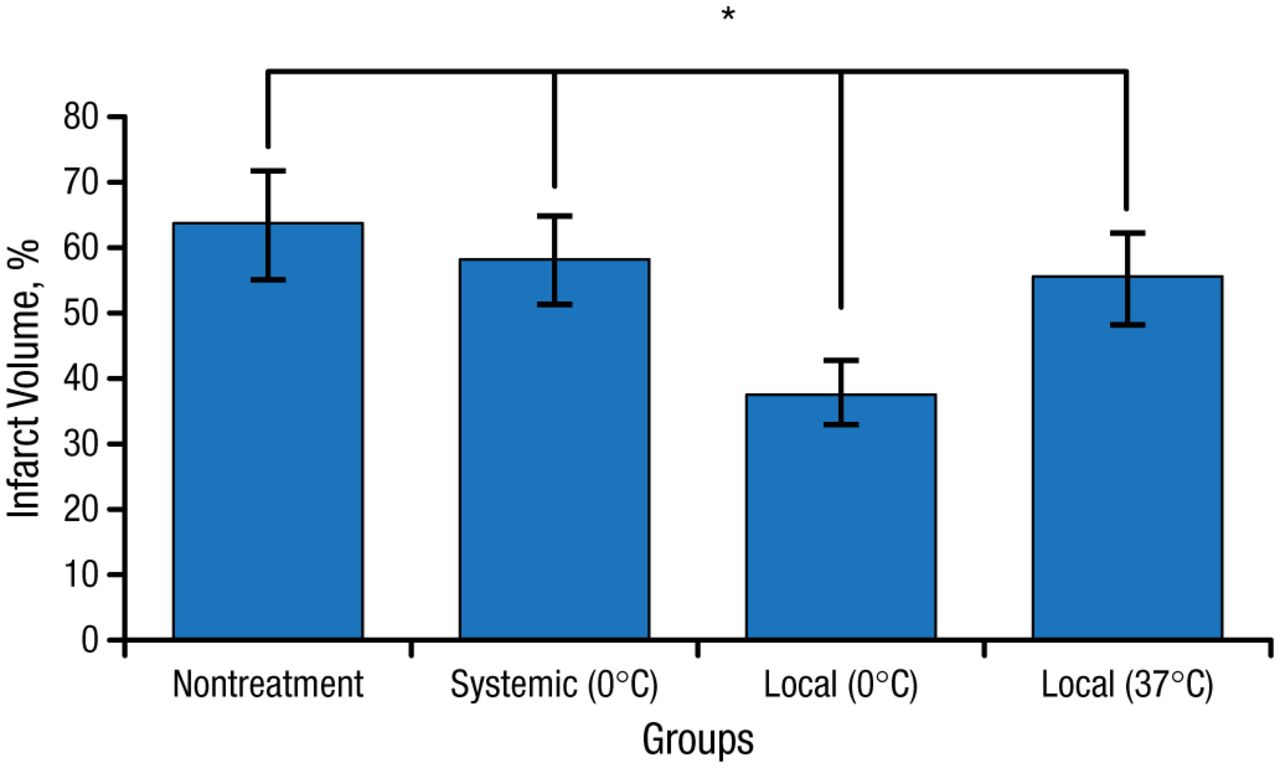
Treatment-Related Differences in Infarct Volume in Rodents
*P < .01
Republished with permission of W. S. Maney & Sons Ltd, from Chen J et al. The effect of a microcatheter-based selective intra-arterial hypothermia on hemodynamic changes following transient cerebral ischemia. Neurol Res. 2015;37:263–268; permission conveyed through Copyright Clearance Center, Inc.
According to Martin Dichgans, MD, University of Munich, Munich, Germany, the extracellular matrix (ECM) and basement membrane (BM) play key roles in cerebral small vessel disease (SVD).
Collagen type IVA1 (COL4A1) protein is abundant in arteries, where it combines with COL4A2 protein, and patients with collagen type IVA–related angiopathies have marked arteriolar BM thickening [Jeanne M et al. Am J Hum Genet. 2012; Verbeek J et al. Eur J Hum Genet. 2012; Gould DB et al. N Engl J Med. 2006].
One form of SVD, known as cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL), is characterized by accumulation of the transmembrane receptor Notch-3 within the ECM of microvessels [Kast J et al. Acta Neuropathol Commun. 2014].
There is also a recessive form of cerebral SVD known as cerebral autosomal recessive arteriopathy with subcortical infarcts and leukoencephalopathy (CARASIL). In this condition, loss of activity of high-temperature-requirement protein A1 (HtrA1) prevents cleavage of latent transforming growth factor-β (TGF-β) binding protein 1 (LTBP-1), resulting in reduced TGF-β signaling [Beaufort N et al. Proc Natl Acad Sci USA. 2014].
Intracerebral hemorrhage (ICH) has historically been seen as the “neglected sibling” of stroke, according to Craig Anderson, MD, PhD, University of Sydney, Sydney, New South Wales, Australia. However, he discussed a recent study that has fortunately changed this perspective [Krishnamurthi RV et al. Lancet Glob Health. 2013]. ICH is the most important subtype of stroke worldwide, responsible for more loss of productive life than ischemic stroke because of its incidence, and because it predominantly affects a younger to middle-aged group of patients who are often in the prime of life.
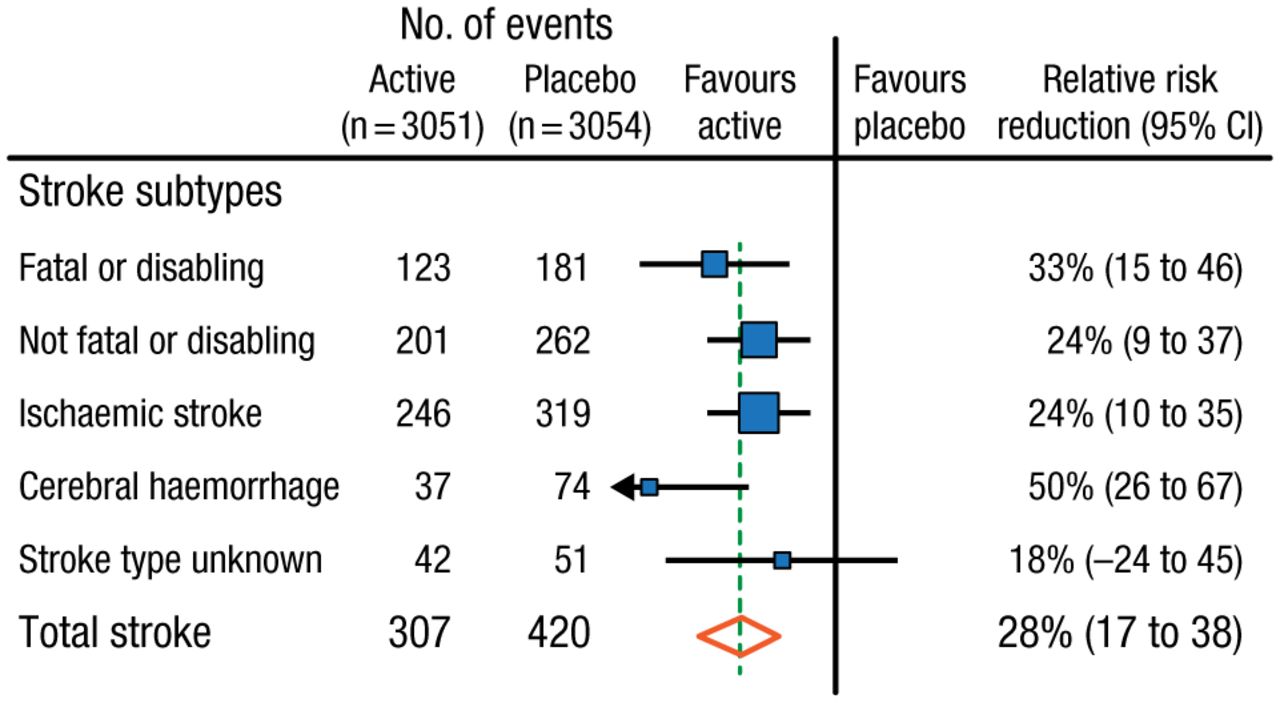
Prof Anderson emphasized the importance of blood pressure (BP) control in ICH management, as demonstrated by the PROGRESS trial [PROGRESS Collaborative Group. Lancet. 2001], which showed that BP reduction benefits patients with ICH more than those with any other stroke subtype (Figure 3).
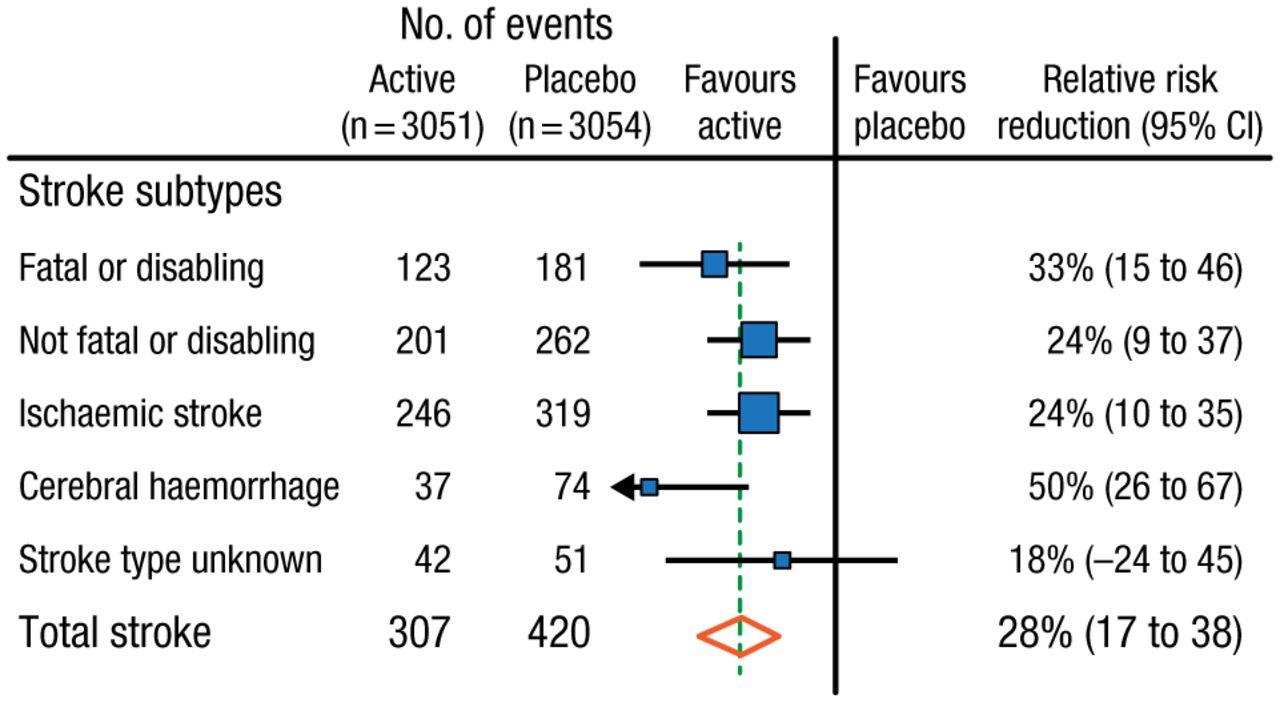
The Effect of Blood Pressure Reduction on Stroke Subtypes
Blue squares = point estimates (with area proportional to number of events); horizontal lines = 95% CIs; diamonds = point estimate and 95% CI for overall effects; vertical broken line = point estimate for overall effect.
Reprinted from The Lancet, PROGRESS Collaborative Group, Randomized trial of a perindopril-based blood-pressure-lowering regimen among 6105 individuals with previous stroke or transient ischaemic attack. 2001;358:1033–1041. Copyright with permission from Elsevier.
On that note, he emphasized the need to improve BP control, highlighting the struggle to help many patients achieve target BP, as well as the recent change in guidelines which has further challenged the situation. Prof Anderson concluded that methods to improve uptake and adherence to BP-lowering treatment are therefore essential, as well as additional strategies, including those that aim to reduce dietary salt intake.
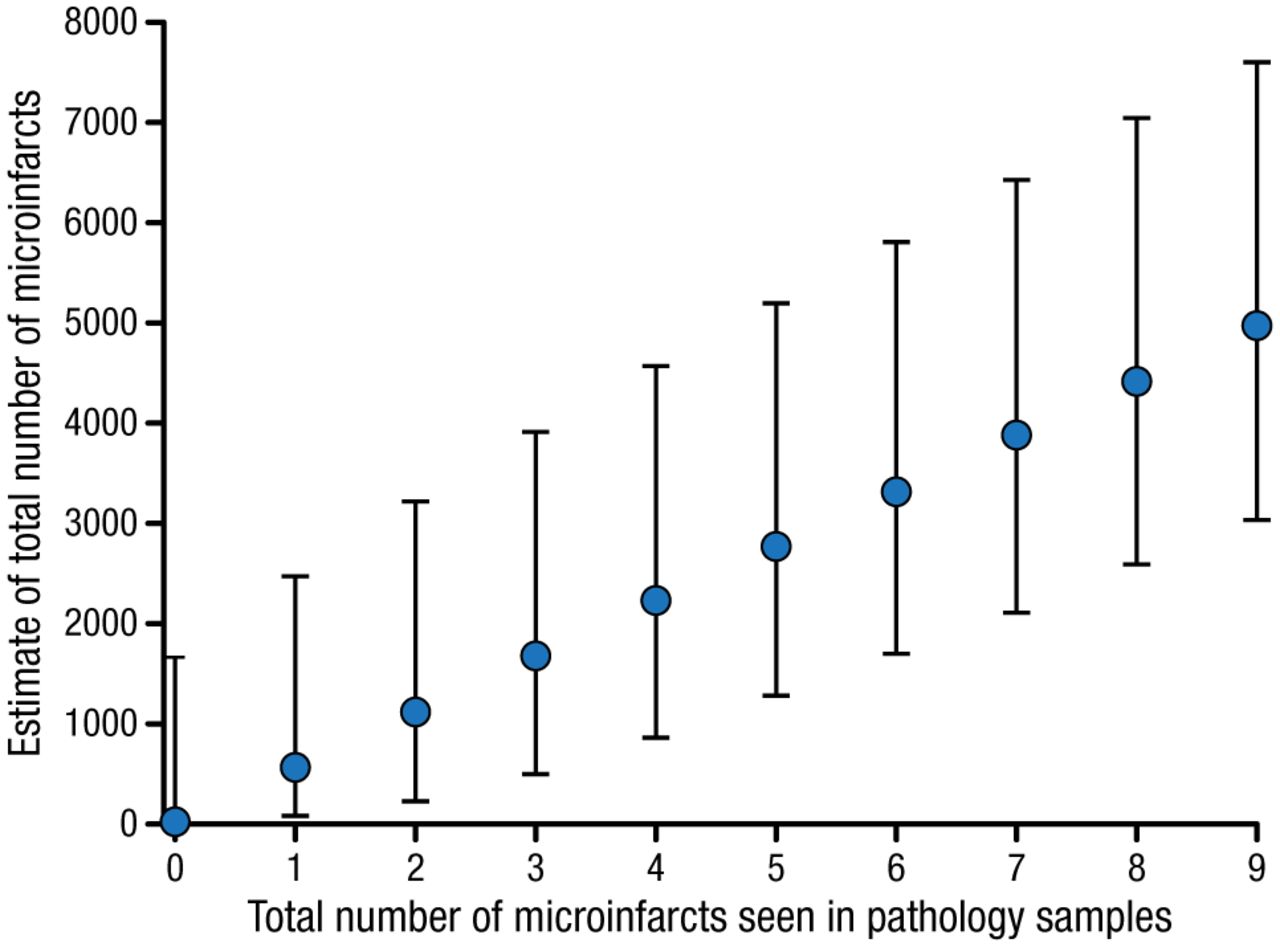
Steven M. Greenberg, MD, PhD, Harvard Medical School, Boston, Massachusetts, USA, stated that there is now overwhelming evidence of the contribution of vascular disease to cognitive impairment. Although brain lesions such as lacunes, cerebral microbleeds, and a mixture of white matter hyperintensities have been associated with cognitive impairment, microinfarcts—areas of tissue loss or cell death with a mean diameter of approximately 200 µm—have been strongly linked to dementia in community-based studies [Smith EE et al. Lancet Neurol. 2012]. However, the small size of microinfarcts is problematic because they are not visible to the naked eye or by magnetic resonance imaging, but are evident only when brain samples are examined microscopically. Nevertheless, data from mathematical models have shown that the presence of even a small number of microinfarcts in a brain sample indicates an abundance of them throughout the whole brain (Figure 4) [Westover MB et al. Neurology. 2013].
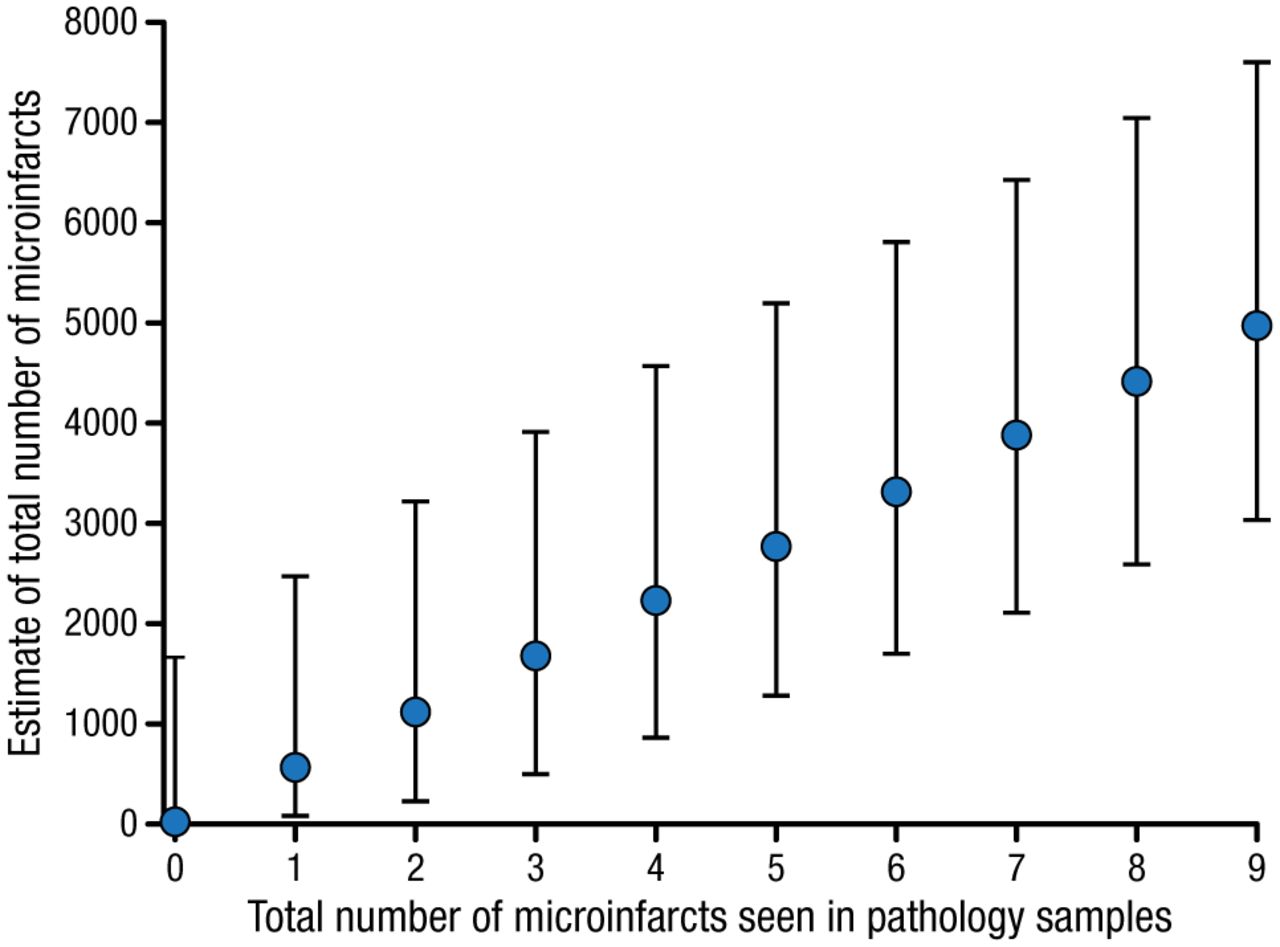
Microinfarct No. in a Brain Sample Correlates With Whole-Brain Microinfarct Burden
Maximum likelihood estimates (blue filled circles) with 90% CIs of the total number of microinfarcts within the brain volume vs total number of microinfarcts seen in routine pathologic specimens.
Reprinted from Westover MB et al. Estimating cerebral microinfarct burden from autopsy samples. Neurology. 2013;80:1365–1369. With permission from American Academy of Neurology.
Dr Greenberg noted that, despite their small size, microinfarcts are true infarcts that cause measureable microstructural changes [Auriel E et al. Neurology. 2014], and represent a strong candidate link between cerebrovascular disease and cognitive impairment. He therefore concluded that further research in this area is essential, potentially by using higher-resolution techniques such as 7 tesla magnetic resonance imaging [van Veluw SJ et al. J Cereb Blood Flow Metab. 2013], or by examining larger-scale measures that might capture the cumulative effects of the lesions such as structural network analysis [Reijmer YD et al. Brain. 2015].
Gert Kwakkel, PhD, University of Amsterdam, Amsterdam, the Netherlands, discussed the role of physical therapy (PT) in evidence-based motor rehabilitation post stroke. He shared data from recent meta-analyses that demonstrate benefit of poststroke PT interventions in restoring activities of daily living in patients [Lohse KR et al. Stroke. 2014; Veerbeek JM et al. PLoS One. 2014]. In particular, Veerbeek and colleagues’ meta-analysis involving 467 trials showed the benefit of high-intensity training in restoring activities of daily living post stroke. However, because patients improve only in those tasks in which they are specifically trained during therapy, Prof Kwakkel emphasized that skill acquisition is mainly driven by the interaction of intensity of therapy and the task and context specificity.
Although it is now widely accepted that more is better with respect to PT post stroke, exactly how much more PT—or even the minimal effective dose—remains unknown, said Prof Kwakkel. Based on evidence-based guidelines, he noted that the worldwide recommended dose of practice ranges from < 30 minutes to > 3 hours per working day, with no evidence for the need to continue exercise therapy on weekends at stroke units, rehabilitation wards, or nursing homes. The challenge for the future is therefore to ensure the accuracy of these guideline recommendations. Appropriately conducted dose–response trials are needed to investigate the same type of therapy with different intensities in different phases after stroke, concluded Prof Kwakkel.
- © 2015 SAGE Publications
Tools









{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.