

Summary
Anesthesia in the severely obese presents unique challenges, including some that are not well understood. This article addresses challenges in anesthesia for obese gynecologic and obstetric patients, as well as the use of antithrombotics and prophylactic antibiotics in patients with obesity, to provide guidance on decision making in these complex cases.
- Obesity
- General Anesthesia
- Obstetrical Anesthesia
- Diagnostic & Surgical Procedures
- Pregnancy
- Anesthesiology
- Obesity
- General Anesthesia
- Obstetrical Anesthesia
- Diagnostic & Surgical Procedures
- Pregnancy
Anesthesia in the severely obese presents unique challenges, including some that are not well understood. Vilma E. Ortiz and Roman Schumann, both members of the International Society for the Perioperative Care of the Obese Patient, addressed challenges in anesthesia for obese gynecologic and obstetric patients, while John L. Walsh addressed the use of antithrombotics and prophylactic antibiotics in patients with obesity, to provide guidance on decision making in these complex cases.
Vilma E. Ortiz, MD, Massachusetts General Hospital, Boston, Massachusetts, USA, presented recommendations on general anesthesia for the obese parturient. Because obesity is common in reproductive–age women (affecting 8%), it is important to be familiar with the physiologic changes associated with pregnancy and obesity to safely administer general anesthesia. Considering that the airway is extremely important for pregnant obese patients, Dr Ortiz focused on airway management. In particular, since general anesthesia is used less frequently for deliveries in the United States, providers have less experience with intubation but may have to accomplish it in emergency, high–stress situations. Special concerns during pregnancy are the possibility of nasal congestion, increase in neck diameter (especially with preeclampsia), and increase in the Mallampati score. It is important to realize that the airway can change not only during pregnancy but also during labor and delivery; one study found that about 33% of patients experienced an increase in their airway classification after delivery [Guru R et al. Anaesthesia. 2013]. In addition, the diaphragm is displaced cephalad by the uterus, decreasing functional reserve capacity and expiratory reserve volume, while there is an increase in oxygen consumption [Hegewald MJ, Crapo RO. Clin Chest Med. 2011]. This raises the risk of rapid desaturation during periods of apnea.
Dr Ortiz outlined 3 important steps that should be followed before induction of general anesthesia in the obese parturient. The first is a thorough evaluation of the airway, with the understanding that it may change, especially after a long labor or with preeclampsia or upper respiratory tract infection. The second is thorough preoxygenation to boost oxygen reserves. Finally, it is important to consider positioning during preoxygenation and induction, as this can have an important influence on oxygenation in the obese.
Roman Schumann, MD, Tufts University School of Medicine, Boston, Massachusetts, USA, used a case study of an obese middle–aged woman requiring anesthesia for a gynecologic procedure to review the respiratory physiology of obese vs lean patients, to discuss ventilation strategies during surgery, and to review decision making for extubation. The patient was a 48–year–old woman with a body mass index (BMI) of 48 kg/m2, type 2 diabetes, and hypertension. The patient had well–managed dyslipidemia (treated with medication) and obstructive sleep apnea (treated using continuous positive airway pressure at night). The surgical procedure (laparoscopic hysterectomy and hiatal hernia repair) required capnoperitoneum and positional changes (reverse Trendelenburg and Trendelenburg), increasing respiratory risks. At the end of the procedure, she showed conjunctival chemosis and subcutaneous emphysema, raising the question of whether immediate postoperative tracheal extubation would be safe.
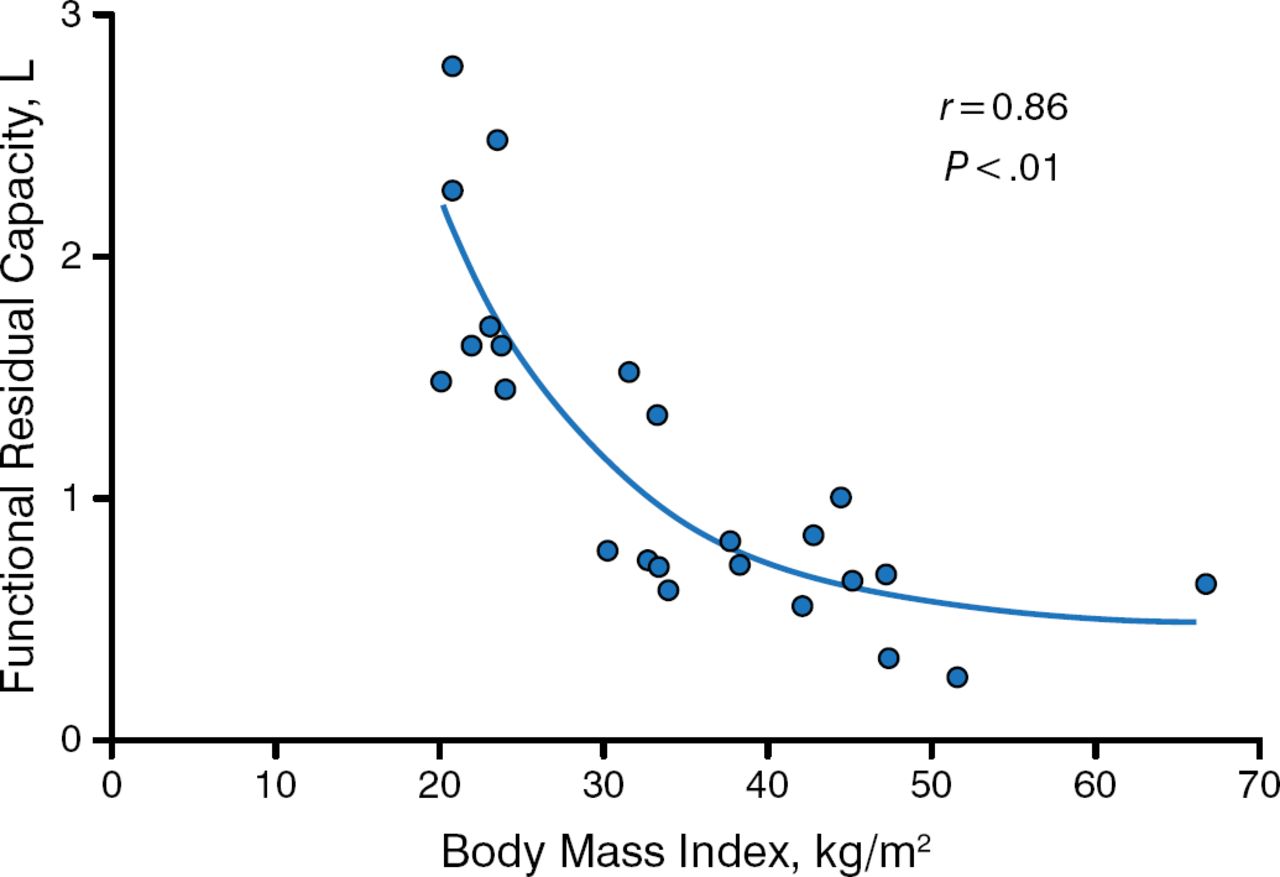
Dr Schumann reviewed some considerations for making the decision, including concerns regarding the respiratory physiology of the obese: a decrease in functional residual capacity (often below the lower limit of normal when the BMI is ≥ 45) and an exponential decrease in oxygenation parallel to the BMI during general anesthesia (Figure 1) [Pelosi P et al. Anesth Analg. 1998]. Additionally, the obese experience increased respiratory resistance (primarily caused by airway or lung resistance) and worse atelectasis immediately after extubation and progressively over the following 24 hours, as compared to lean patients, who are typically improving during this time. Intraoperative peak inspiratory pressure can increase substantially.

Functional Residual Capacity Decreases Parallel to Body Mass Index
Reprinted from Anesth Analg, 87, Pelosi P et al. The effects of body mass on lung volumes, respiratory mechanics, and gas exchange during general anesthesia, Copyright 1998, with permission from International Anesthesia Research Society.
While positive end–expiratory pressure and recruitment maneuvers improve oxygenation, much is still uncertain about the best way to use these intraoperative interventions in obese patients (eg, frequency and specific mechanics of recruitment maneuver administration) [Reinius H et al. Anesthesiology. 2009]. Additionally, adipose tissue is metabolically active, consuming oxygen and producing carbon dioxide, but severely obese individuals have restrictive respiratory physiology and can have substantial respiratory muscle dysfunction (causing a ≤ 50% decrease in breathing efficiency) [Koenig SM. Am J Med Sci. 2001]. Work of breathing can substantially increase at baseline for obese versus the nonobese (≤ 280% in metabolically impaired patients).
Specific recommendations for the case study patient included maintaining a reverse Trendelenburg position of ≥ 30° when possible, using recruitment maneuvers followed by positive end–expiratory pressure, and using care to respond to hemodynamic responses with appropriate maneuvers [Aldenkortt M et al. Br J Anesth. 2012]. Applying this extrapolated evidence from the literature, Dr Schumann explained that this patient was not extubated in the operating room. Instead, she was allowed to demonstrate that she could generate the necessary work of breathing and eliminate excess (subcutaneous) carbon dioxide before safe extubation in the recovery room.
In addition to these discussions of anesthesia in obese patients, John L. Walsh, MD, Massachusetts General Hospital, Boston, Massachusetts, USA, contributed to the session with a discussion of recommendations for the use of antithrombotics and antibiotics, focusing on dosing and monitoring recommendations along with the supporting evidence.
Dr Walsh reviewed common perioperative antithrombotic agents, explaining the mechanisms of action of unfractionated heparin, low–molecular–weight heparin (LMWH), and fondaparinux. Because unfractionated heparin can cause bone resorption and because fondaparinux is sufficiently small to pass through the placenta, LMWH (which does not cross the placenta) is the anticoagulant of choice for indicated prophylaxis of venous thromboembolism in pregnant women. Other antithrombotic alternative medications are either known to cause problems in pregnancy (eg, Coumadin) or have not been sufficiently studied to be considered safe.
The American College of Obstetricians and Gynecologists and the American College of Chest Physicians issued consistent practice guidelines in 2011 and 2012 regarding the use of antithrombotics [James A et al. Obstet Gynecol. 2011; Bates SM et al. Chest. 2012]. These guidelines, which match the recommendation of the package insert, advise obtaining anti–Xa levels for pregnant as well as obese patients to monitor and tailor management. However, the assays vary considerably, and it is critical to understand the assays being used and their normal ranges to interpret the results. An assay of heparin level in the blood is not the same as an assay of anticoagulation in the blood; LMWH must bind to antithrombin to work, and it is ineffective in patients with antithrombin deficiency or other causes of low antithrombin levels (eg, a recent clot). Assays that use endogenous antithrombin in plasma are anticlotting assays rather than heparin assays.
While it is often necessary to know if patients are receiving a therapeutic dose of LMWH for prophylaxis, it is also important to know how to proceed when patients receiving LMWH need procedures that could result in bleeding. The American Society of Regional Anesthesia and Pain Medicine issued guidelines for this situation [Horlocker TT et al. Reg Anesth Pain Med. 2010]. A recent population pharmacokinetic model suggests that these guidelines are safe for the morbidly obese because clearance is faster in obese patients [Diepstratenm J, http://hdl.handle.net/1887/209592013].
Dr Walsh also addressed perioperative antibiotic usage in the obese population, beginning with guidelines for antimicrobial prophylaxis from the Infectious Diseases Society of America, the American Society of Health–System Pharmacists, the Surgical Infection Society, and the Society for Healthcare Epidemiology in America. For 34 of the 38 procedures listed, cefazolin was the recommended medication. The consensus statement recommended pediatric weight–based doses of 30 mg/kg and 2 or 3 g (for adults > 80 kg or > 120 kg, respectively) [Bratzler DW et al. Am J Health Syst Pharm. 2013]. However, when interpreting and appraising the current literature, one needs to understand the differences between antibiotic concentration found in cells versus the interstitial fluid.
In conclusion, new insights and methodologies reported in dosing studies resulted in the upward adjustment of the recommended prophylactic doses for some antibiotics, and these higher doses appear to be safe (Table 1). Dr Walsh concluded that these higher doses should be used to achieve sufficient therapeutic concentrations within the body.
Recommended Weight–Based Doses
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.