

Summary
Combined injury to the anterior cruciate ligament (ACL) and meniscus is a common sports-related injury. A frequent outcome of this injury is posttraumatic osteoarthritis (PTOA), a devastating condition for young patients [Smith JP III et al. Am J Sports Med 2001]. Over the past 3 decades, treatment of this type of injury has focused on meniscus preservation to improve outcomes and possibly prevent PTOA [Stein T et al. Am J Sports Med 2010].
- Orthopaedic Procedures Clinical Trials
- Sports Medicine
- Hip & Knee Conditions
- Orthopaedic Procedures
- Orthopaedics Clinical Trials
- Sports Medicine
- Orthopaedics
- Hip & Knee Conditions
Combined injury to the anterior cruciate ligament (ACL) and meniscus is a common sports-related injury. A frequent outcome of this injury is posttraumatic osteoarthritis (PTOA), a devastating condition for young patients [Smith JP III et al. Am J Sports Med 2001]. Over the past 3 decades, treatment of this type of injury has focused on meniscus preservation to improve outcomes and possibly prevent PTOA [Stein T et al. Am J Sports Med 2010].
Robert W. Westermann, MD, University of Iowa, Iowa City, Iowa, USA, reported an 86% success rate at 6 years among patients receiving concurrent ACL reconstruction (ACLR) and meniscus repair [Westermann RW et al. Am J Sports Med 2014]. The study was based on data from the Multicenter Orthopedic Outcomes Network (MOON) database. Surgeon and patient questionnaires for the years 2002 to 2004, as well as operative reports for subsequent knee surgery, were analyzed with Microsoft Excel and SPSS software at entry and again at 2 and 6 years. Meniscus repair failure was defined as a need for subsequent meniscus surgery by debridement, excision/meniscectomy, or revision repair.
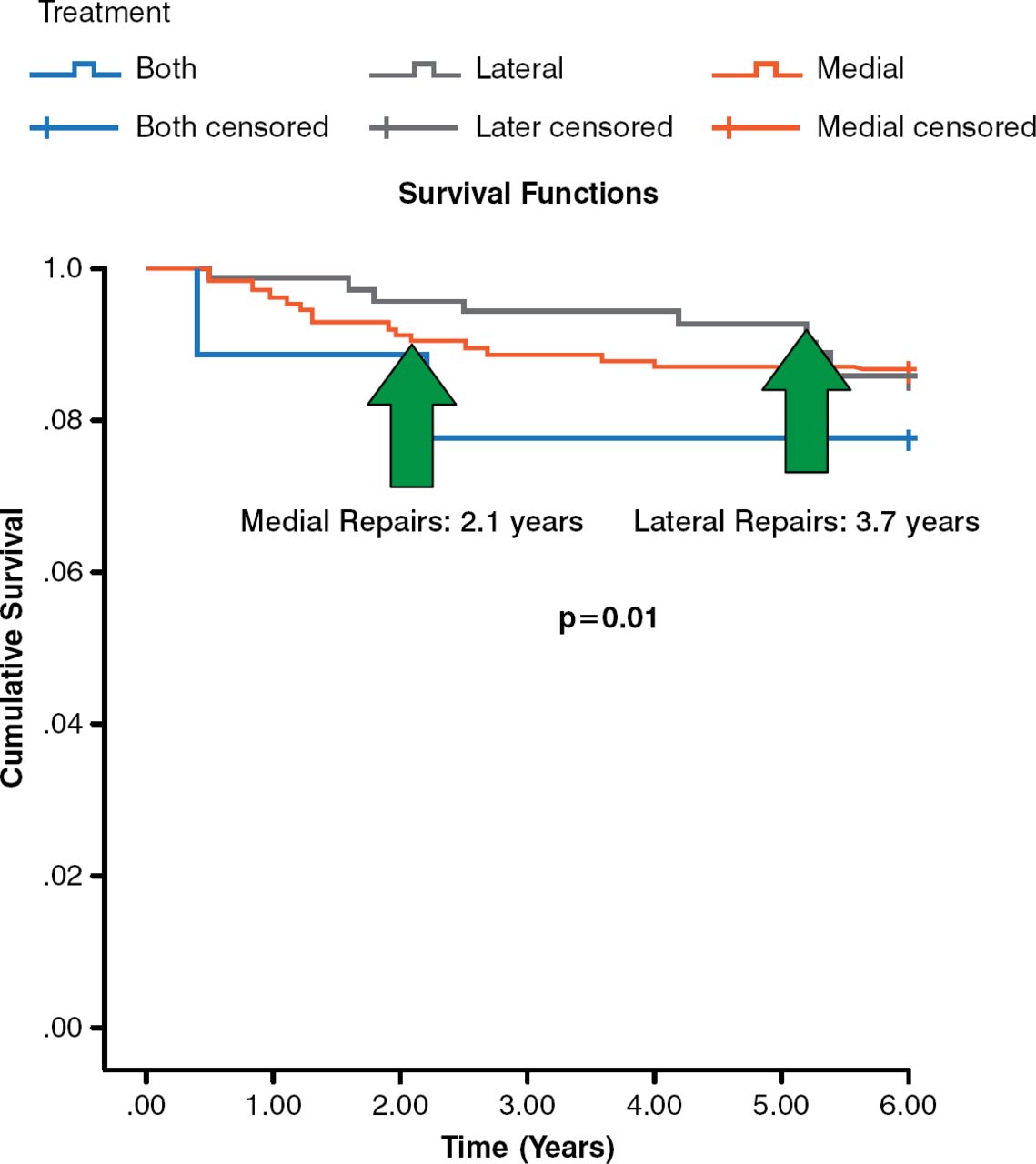
Primary ACLR was performed in 1440 patients, 286 of whom underwent concurrent meniscus repair. Most patients (n = 235 of 286; 82.2%) were available for follow-up at 6 years (n = 154, medial; n = 72, lateral; n = 9, both medial and lateral). There were no differences between successful and failed repairs regarding tear pattern (84% longitudinal), location (10% displaced bucket handle), or size (mean, 16.5 ± 5.8 mm). Of the 154 medial meniscus repairs, 21 (13.6%) were failures. There were 10 failures among patients with lateral repairs (n = 10 of 72; 13.9%). The failure rate for both medial and lateral repair was 22.2% (n = 2 of 9). Mean time to failure of medial repairs was 2.1 years, compared with 3.7 years for lateral repairs (p = .01; Figure 1).

Time to Medial and Lateral Repair Failure
Note that medial repairs appeared to fail early (2.1 years), while lateral repair failures more commonly occurred late (3.7 years).
Reproduced from Westermann RW et al. Meniscal repair with concurrent anterior cruciate ligament reconstruction operative success and patient outcomes at 6-year follow-up. Am J Sports Med 2014; DOI: 10.1177/0363546514536022. Copyright © 2014 American Orthopaedic Society of Sports Medicine.
At 6 years, lower failure rates were noted with inside-out procedures (n = 19 patients), compared with the all-inside technique (n = 208 patients): 5.3% (n = 1) versus 14.9% (n = 31), respectively. Patient numbers were too low to detect a significant difference, however.
Patient-reported outcomes were assessed with the Knee injury and Osteoarthritis Outcome Score. Patients receiving medial and lateral repairs had similar improvements, which were significant at 2 years and maintained out to 6 years (p value not shown). A single subscore (knee-related quality of life) identified patients who received bilateral repairs and those who had failed lateral meniscus repair as being worse at their 6-year follow-up. About 40% of these repair failures were associated with a primary ACLR failure.
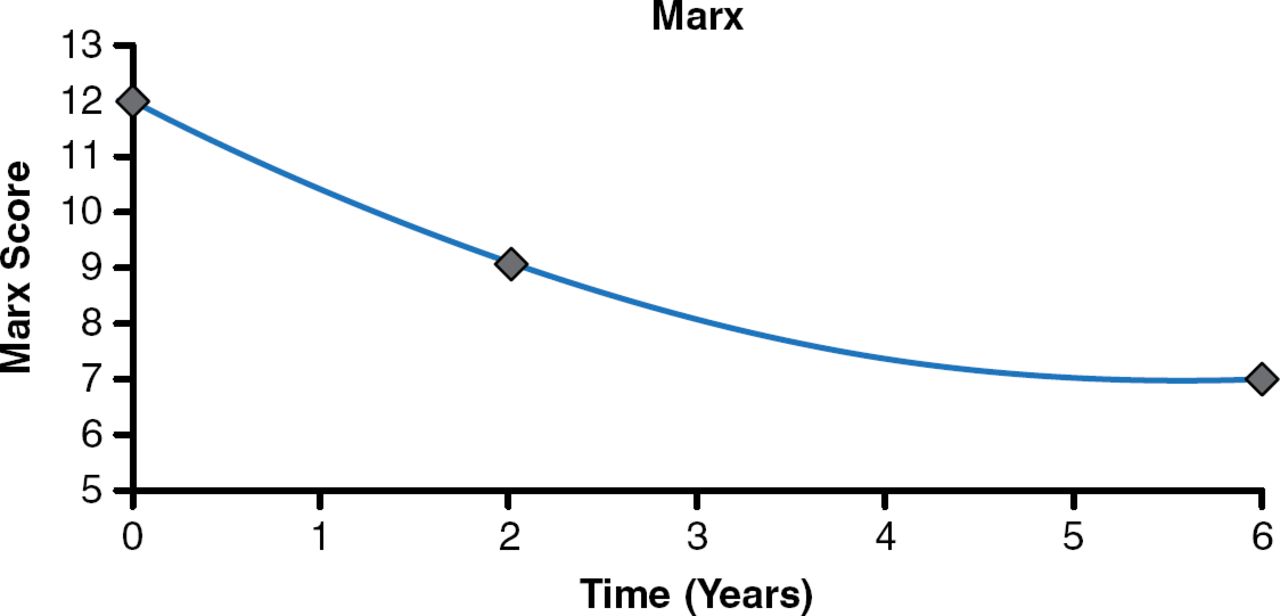
Activity level, as defined by the Marx Activity Scale, decreased over time (Figure 2). There were no differences in number or type of sutures or repair device between repair failures and successes. An increase in subsequent knee surgery was noted among patients receiving meniscus repair compared with those with uninjured meniscus.

Marx Activity Scores Decreases Over Time
Marx score correlates with activity level and returning to pivoting sports.
Reproduced with permission from RW Westermann, MD.
Several factors influence patient outcomes after ACLR. MOON data reported by Cox and colleagues [Am J Sports Med 2014] indicate that ACL revision, meniscus or chondral injury, and medial meniscus repair are predictors of poor outcomes. In this large study of patients with ACLR plus meniscus repair, medial and lateral repairs had similar failure rates and similar patient outcomes, which were significant at 2 years and well maintained out to 6 years.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.