

Summary
About 16% of all fractures treated by orthopaedic surgeons are of the distal radius, and the most common procedure used for their treatment is open reduction and internal fixation. Data from Brachial Plexus Block in Post-Op Pain Control After Distal Upper Extremity Fracture: A Prospective, Randomized Study [NCT01968824] compared the use of general anesthesia and brachial plexus blockade. Results are discussed in this article.
- Pain Management
- Acute & Chronic
- Orthopaedic Pain Management
- Orthopaedic Procedures
- Orthopaedics Clinical Trials
- Conduction Anesthesia
- Hand & Wrist Conditions
- General Anesthesia
- Pain Management
- Acute & Chronic
- Orthopaedic Pain Management
- Orthopaedics
- Orthopaedic Procedures
- Orthopaedics Clinical Trials
- Conduction Anesthesia
- Hand & Wrist Conditions
- General Anesthesia
Preoperative pain control with brachial plexus blockade (BPB) reduced the need for other analgesics in the postanesthesia care unit (PACU); however, rebound pain caused greater pain scores postdischarge compared with patients who received general anesthesia (GA) during surgical fixation of distal radius fracture. Nirmal C. Tejwani, MD, New York University Langone Medical Center, New York, New York, USA, presented data from Brachial Plexus Block in Post-Op Pain Control After Distal Upper Extremity Fracture: A Prospective, Randomized Study [NCT01968824].
About 16% of all fractures treated by orthopaedic surgeons are of the distal radius, and the most common procedure used for their treatment is open reduction and internal fixation (ORIF). Currently, there are 2 methods of surgical anesthesia: GA and BPB; however, there are few studies that have evaluated their efficacy in surgeries that treat injuries distal to the elbow. Advantages of BPB are thought to include muscle relaxation and greater hemodynamic stability, as well as reduced PACU time, postoperative pain, and opioid use, decreased readmission for pain control, and increased patient satisfaction compared with GA. The purpose of this study was to evaluate the use of BPB in patients undergoing operative fixation of distal radius fracture.
In this prospective trial, 36 patients with closed distal radius fractures requiring operative fixation were enrolled and were randomly assigned to receive GA or BPB pre-operatively. Patients were excluded from the study if they had an open fracture or medical comorbidities, or if they refused. Oxycodone (5 mg) plus acetaminophen (325 mg) was administered to all patients on discharge. Follow-up occurred at 2, 4, 6, 12, 24, 48, and 72 hours postoperation to evaluate pain scores according to the visual analog scale and the number of pain tablets ingested.
The primary outcome of the study was pain scores. Secondary outcomes included time in the PACU, total pain medication required in the PACU, patient satisfaction, and functional outcome scores of the Disabilities of the Arm, Shoulder, and Hand (DASH) outcome measure and Short Musculoskeletal Function Assessment (SMFA).
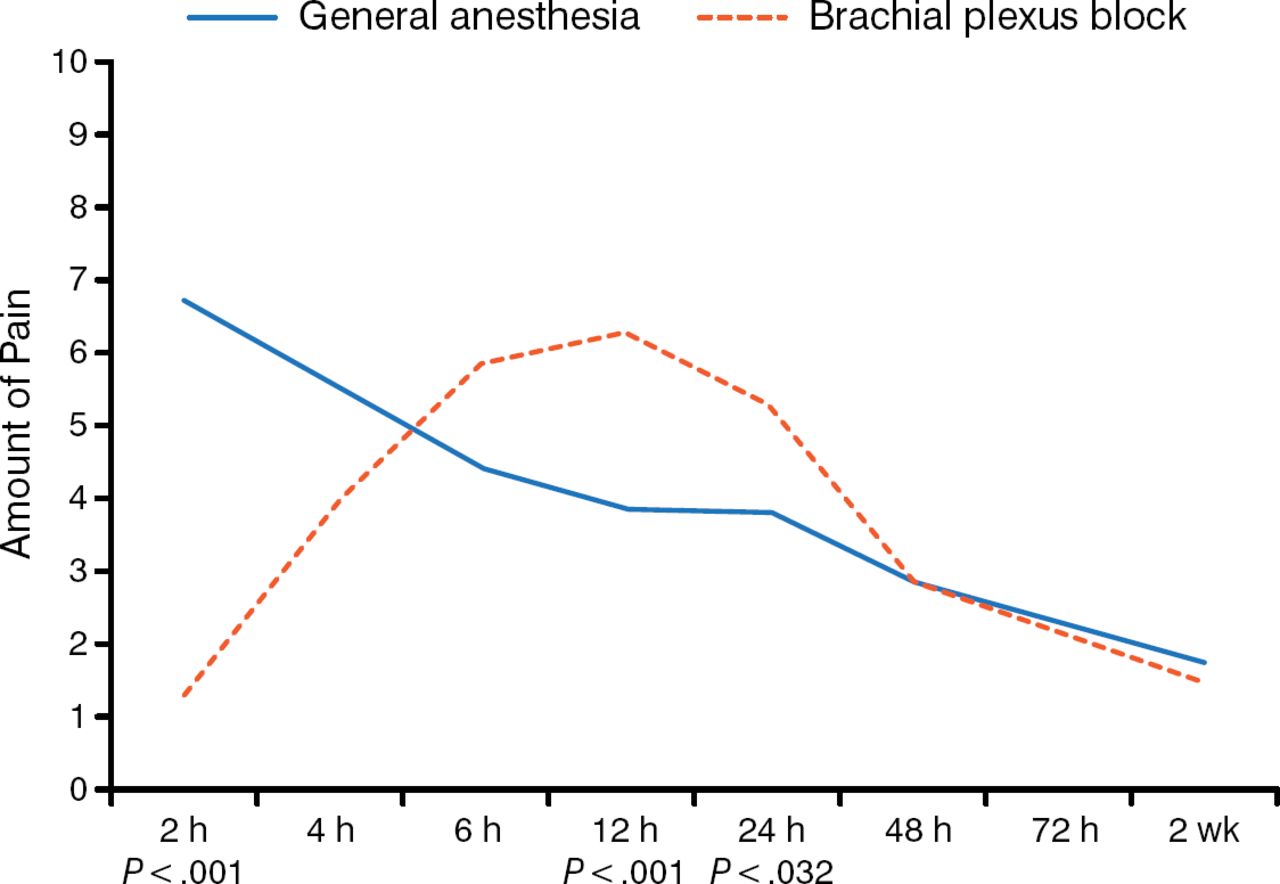
At 2 hours, the BPB arm demonstrated significantly less pain compared with the GA arm (P < .001); however, at 12 and 24 hours, the BPB arm demonstrated significantly greater pain compared with the GA arm (P < .001 and P = .032, respectively), which then decreased to similar levels as the GA arm at 48 hours, 72 hours, and 2 weeks (Figure 1).

Pain Associated With Brachial Plexus Block During Distal Radius Fracture Fixation
Reproduced with permission from NC Tejwani, MD.
Patients who received BPB required significantly less time in the PACU compared with patients who received GA (197 minutes vs 284 minutes; P = .026). In addition, patients in the GA group required significantly more fentanyl (P = .003) and morphine compared with patients in the BPB group. However, there was no significant difference in functional outcome scores or oxycodone-acetaminophen consumption postdischarge. There was a trend of greater patient satisfaction in the GA arm compared with the BPB arm, although it was not significant (P = .279).
In conclusion, Dr Tejwani highlighted that although there are multiple benefits of BPB for postoperative pain control in patients undergoing fixation of distal radius fracture, rebound pain can occur. Therefore, use of GA may be beneficial in these patients. The orthopaedic surgeon should educate patients on the benefits of BPB and GA to determine the best pain management option.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.