

Summary
This article discusses revision strategies for ankle and hindfoot treatment. Specific topics include supramalleolar osteotomy for the treatment of ankle osteoarthritis, tibiotalocalcaneal fusion using the retrograde intramedullary (IM) nail for complex hindfoot problems, strategies for surgical treatment of hindfoot valgus and varus deformities, as well as hindfoot malalignment with soft tissue concerns.
- Foot & Ankle Conditions
- Orthopaedic Procedures
- Bone Density & Structure Disorders
- Arthritis
- Foot & Ankle Conditions
- Orthopaedic Procedures
- Orthopaedics
- Bone Density & Structure Disorders
- Arthritis
This symposium featured 4 presentations covering revision strategies for ankle and hindfoot treatment. The first presentation reviewed evidence for the treatment of ankle osteoarthritis (OA) with supramalleolar osteotomy (SMOT). The second presentation focused on tibiotalocalcaneal (TTC) fusion using the retrograde intramedullary (IM) nail for complex hindfoot problems. Strategies for surgical treatment of hindfoot valgus and varus deformities were described in the third presentation. The final speaker presented case studies of unique hindfoot malalignment with soft tissue concerns, detailing clinical features, diagnosis, and treatment options.
SUBSTANTIAL PAIN RELIEF AND FUNCTIONAL IMPROVEMENT WITH SMOT
Alexej Barg, MD, University Hospital of Basel, Basel, Switzerland, discussed the assessment and treatment options for ankle OA. Most patients with deformities of the distal tibia and fibula are younger and have posttraumatic OA. Concomitant problems often include instabilities, muscular dysbalances, and adjacent joint pathologies. Treatments include joint-preserving surgery (JPS) and joint replacement options. The option chosen depends on the complications and stage of ankle OA.
Ankle OA causes an asymmetric joint load and asymmetric cartilage damage. The varus ankle is a complex problem with medialized pull of the heel cord, overload of the medial ankle and lateral ankle ligaments, and overstress of the peroneus brevis tendon. The valgus ankle results in lateralized pull of the heel cord, overload of the lateral ankle and medial ankle ligaments, and overstress of the syndesmotic ligaments.
The primary aims of realignment surgery are osseous and ligamental balancing and restoration of ankle and hindfoot biomechanics. Preoperative assessment includes conventional radiography and single-photon emission computed tomography.
Dr Barg's group treated 42 patients with asymmetric ankle OA: 26 with valgus deformity and 16 with varus deformity [Barg A et al. Tech Foot Ankle Surg. 2013]. Anterior ankle arthroscopy was performed in 35 of these patients. Valgus deformities were treated with medial closing wedge osteotomy (OT) (n = 26). Varus deformities were treated with medial opening wedge OT (n = 11) or lateral closing wedge OT (n = 5). At a mean follow-up of 4.8 years, the medial distal tibial angle changed from 84.6° ± 7.0° to 91.2° ± 6.1° in the varus group and from 93.5° ± 7.0° to 88.8° ± 4.4° in the valgus group. Visual Analog Scale (VAS) pain scores changed from 5.2 ± 2.6 to 2.6 ± 1.8. SMOT failed in 4 patients.
Potential complications of ankle JPS can include injury of neurovascular tendons or structures, infection, wound healing problems, delayed union or nonunion, patient noncompliance with rehabilitation, and progression of OA in up to 25% of ankles.
Realignment surgery with SMOT demonstrated substantial pain relief and functional improvement in clinical trials. Complications occurred in up to 25% of patients.
HIGH SUCCESS RATE WITH TTC FUSION USING THE IM NAIL IN COMPLEX HINDFOOT PROBLEMS
Complex hindfoot problems that present a challenge for foot and ankle surgeons include Charcot arthropathy, failed total ankle arthroplasty (TAA), ankle and subtalar joint OA, and other deformities. The goal of treatment, regardless of cause, is to realign the foot. Jin Woo Lee, MD, PhD, Yonsei University College of Medicine, Seoul, Korea, discussed implant options for repair of these disorders.
Implant choices include a cannulated screw, locking plate, external fixator (EF), and retrograde IM nail. Prof Lee prefers TTC fusion with the IM nail because it provides biomechanical stability compared with the EF [Fragomen AT et al. Foot Ankle Int. 2008], the lag screws [Berend ME et al. Foot Ankle Int. 1997], and the locking plate [O'Neill PJ et al. Foot Ankle Int. 2008]. The IM nail allows one-stage correction of deformity [Kane JM et al. J Bone Joint Surg Br. 2014] and results in a high union rate [Rammelt S et al. Foot Ankle Int. 2013; Mückley T et al. Foot Ankle Int. 2011].
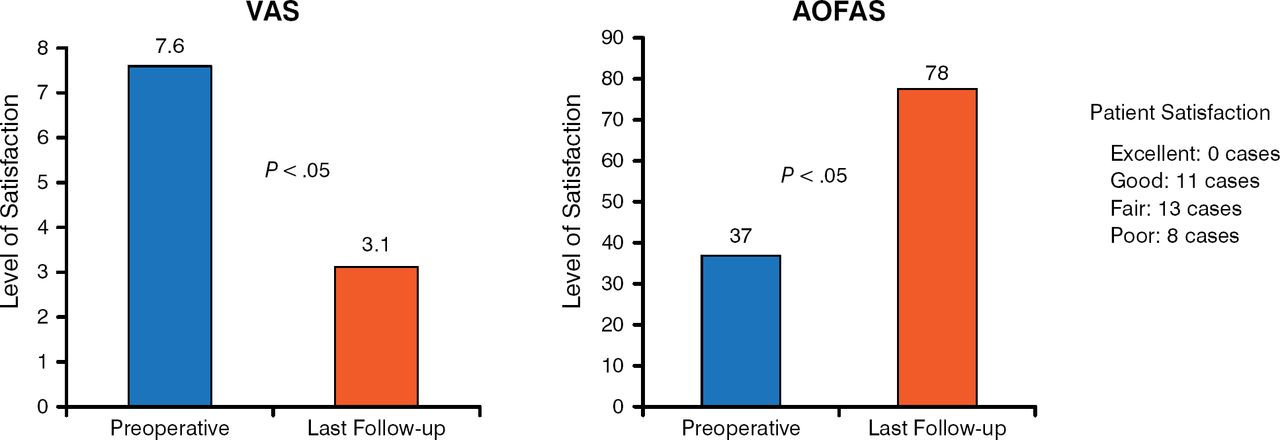
Over 4 years, Prof Lee performed TTC fusion with the retrograde IM nail in 34 cases (32 patients). At a mean follow-up of 48 months, the overall union rate was 82% and the union duration was 7.6 months (Table 1).
Union Status by Cause
Improvements in the VAS and American Orthopaedic Foot & Ankle Society scores were statistically significant (P < .05; Figure 1) from preoperation to last follow-up.

Clinical and Patient Satisfaction Outcomes
AOFAS, American Orthopaedic Foot & Ankle Society; VAS, Visual Analog Scale.
Reproduced with permission from JW Lee, MD.
Major complications occurred in 23.5% of cases. The failure rate was high in patients with uncontrolled diabetes (71%) vs all others (11%; P = .004).
TTC fusion with the retrograde IM nail offers a chance for successful salvage of complex hindfoot problems. However, there is an increased risk of failure in patients with uncontrolled DM.
STRATEGIES FOR SURGICAL TREATMENT OF HINDFOOT VALGUS AND VARUS DEFORMITIES
Emilio Wagner, MD, Clinica Alemana, Santiago, Chile, discussed revision strategies for the correction of hindfoot misalignments. Evaluation of hindfoot deformities includes checking for underlying causes, identifying the origin, checking joint status and stiffness, and assessing midfoot compensation. The initial approach to treatment of valgus and varus deformities consists of conservative strategies, including weight and activity modification, orthotics, and physical therapy.
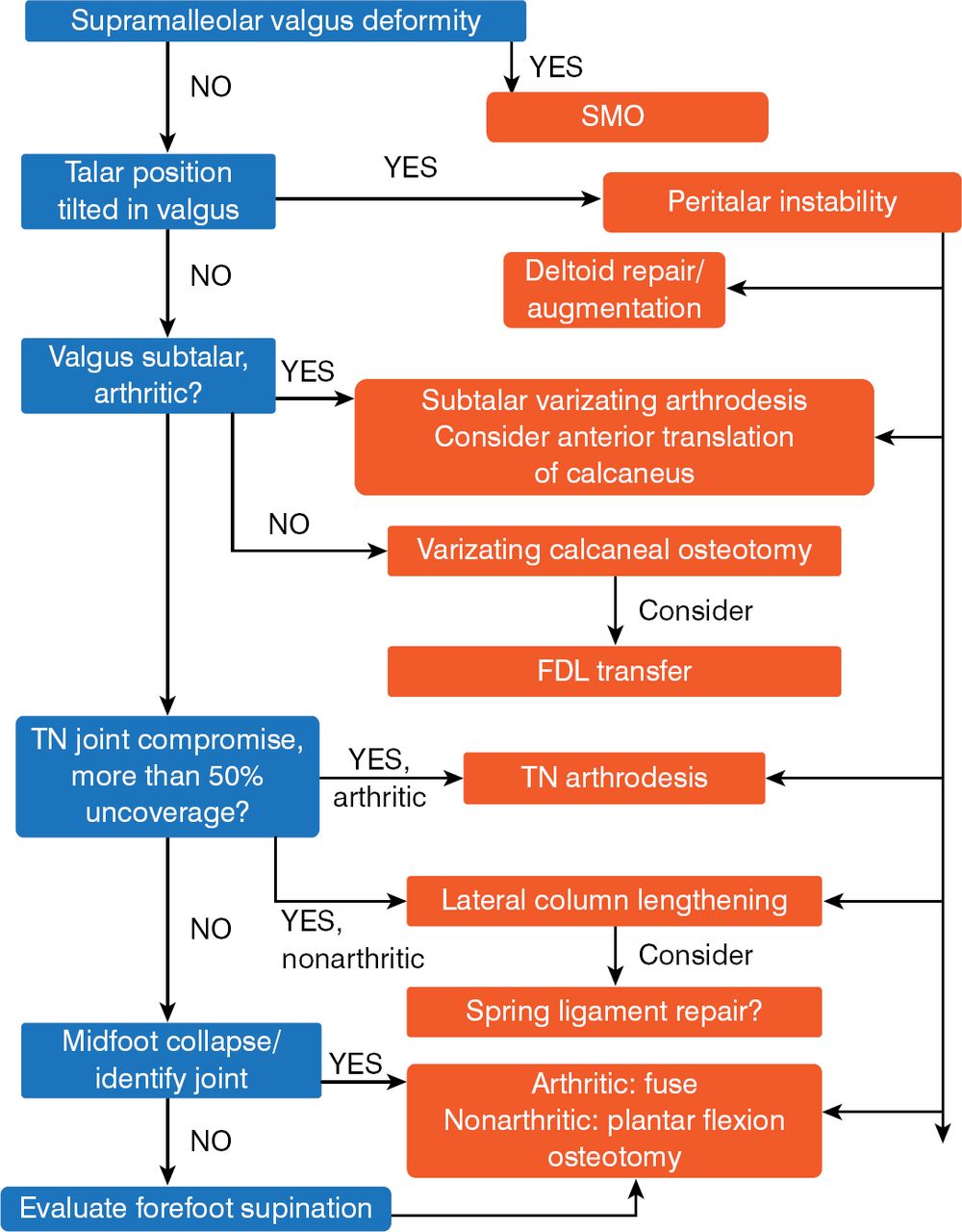
Figure 2 presents an algorithm for surgical treatment of hindfoot valgus deformities.

Hindfoot Reconstruction for Valgus Deformities
FDL, flexor digitorum longus; SMO, supramalleolar osteotomy; TN, talonavicular.
Reproduced with permission from E Wagner, MD.
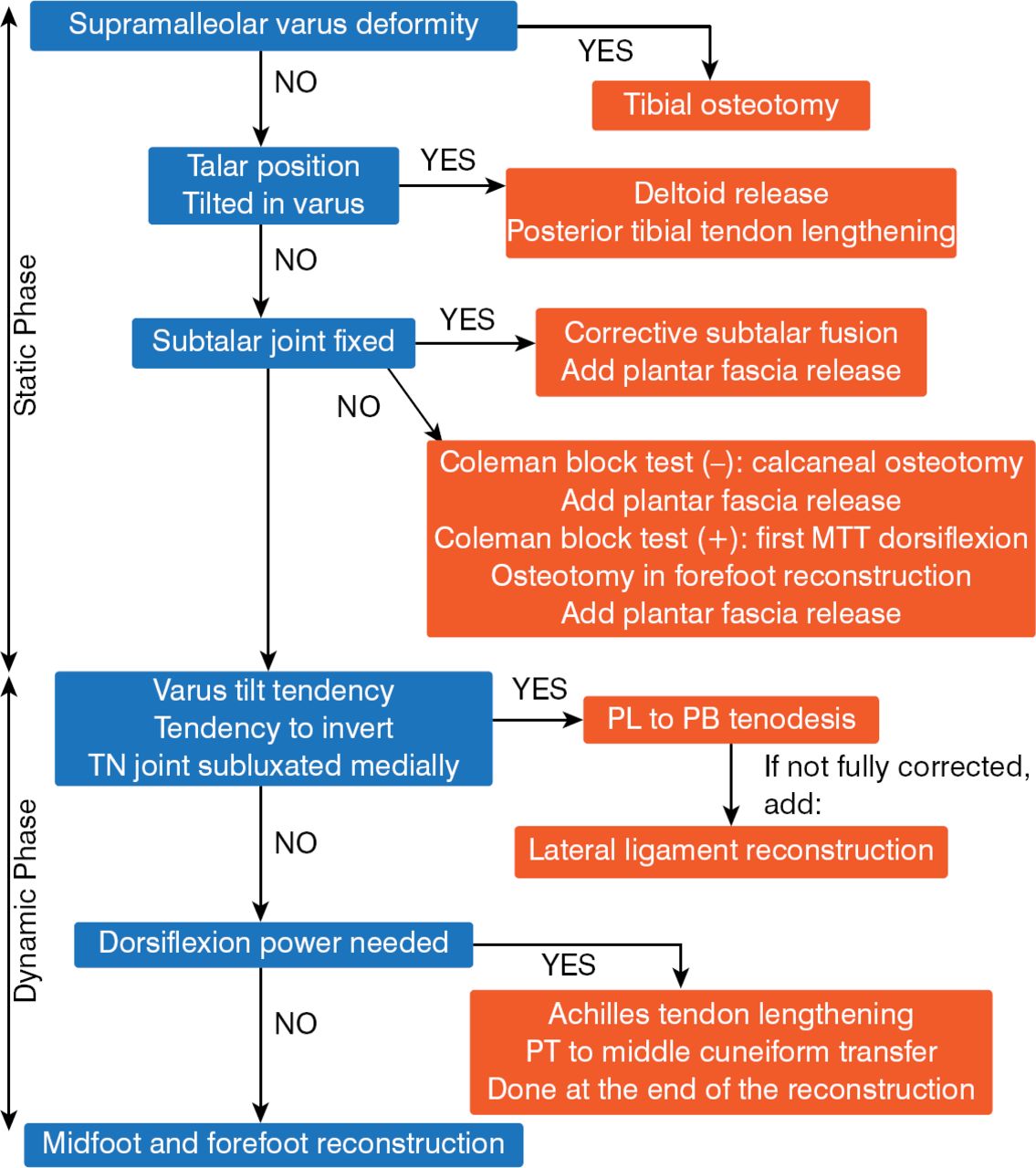
Figure 3 shows an algorithm for surgical treatment of hindfoot varus deformities.

Hindfoot Reconstruction for Varus Deformities
MTT, manual talar tilt; PB, peroneus brevis; PL, peroneus longus; PT, posterior tibial.
Reproduced with permission from E Wagner, MD.
Case Studies
For surgical treatment of hindfoot valgus, Prof Wagner recommended taking the alignment to a slight varus. Fusion may be necessary to achieve stability. For hindfoot varus, additional transfers or releases should be considered to regain ankle stability.
UNIQUE TREATMENT FOR UNIQUE HINDFOOT MALALIGNMENT WITH SOFT TISSUE CONCERNS
Mark Glazebrook, PhD, MD, Queen Elizabeth II Health Sciences Centre, Halifax, Nova Scotia, Canada, reviewed treatment strategies for unique cases of hindfoot malalignment with soft tissue concerns. Hindfoot deformity can be caused by progressive motor sensory conditions such as Charcot-Marie-Tooth disease, nonprogressive disorders such as cerebral palsy and poliomyelitis, and traumatic injuries. Evaluation includes taking a history to determine the source of pain, functional limitations, trauma history, and previous treatments. Physical examination of the standing gait and location of the deformity is important, as is neurologic examination, especially in progressive conditions. Examination also includes assessment of deformity flexibility or rigidity, Achilles length, leg-length discrepancy, and a Coleman block test. Other assessments include diagnostic imaging and electrodiagnostic tests.
According to Prof Glazebrook, a good clinical approach is needed when managing unique cases of hindfoot malalignment with soft tissue concerns; unique cases require unique treatment.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.