

Summary
This article discusses the use of periarticular osteotomy for the treatment of tibial malalignment, ankle distraction, ankle fusion, as well as the pharmacological options for treating ankle osteoarthritis.
- Arthritis
- Foot & Ankle Conditions
- Orthopaedic Procedures
- Arthritis
- Foot & Ankle Conditions
- Orthopaedics
- Orthopaedic Procedures
Open reduction internal fixation has traditionally been the standard approach for treatment of tibial pilon fractures. Although the results with this approach have improved over time, a high rate of complications remains and continues to affect long-term outcomes (eg, nonunion, delayed union, malunion, and infection). Regardless of the cause, malalignment of the tibia can alter ankle mechanics and affect other joints and structures, including the knee and hip. Donald R. Bohay, MD, Michigan State University, East Lansing, Michigan, USA, discussed the use of periarticular osteotomy for the treatment of tibial malalignment.
According to Dr Bohay, preoperative preplanning for periarticular osteotomy should include attention to prior surgical scars, adhesions, infection history, and vascular insufficiency, all of which may influence outcomes. A thorough structural evaluation should focus on assessing maximal deformity as defined from the center of rotation and angulation. Clinical examination should include patient comorbidities such as diabetes and smoking history and leg-length measurement, which may help to determine which type of osteotomy to perform. To avoid malalignment, close attention should be paid to internal and external rotation and the tibial tubercle should be aligned to the second toe. The tibial tubercle should then be compared with the uninvolved limb and the subtalar and Chopart joint motion should be assessed. Computed tomography may help with deformity analysis and assessment of joint health. Fixation options include low-profile plates, locking plates, crossed screws, and external fixation. Potential complications include soft-tissue healing when operating through old scars, delayed union, nonunion, and translational malalignment.
According to Douglas N. Beaman, MD, Summit Orthopedics, Portland, Oregon, USA, ankle distraction is the application of a joint-preserving apparatus that increases joint space, allows weightbearing and motion, and remains in place for months. Dr Beaman pointed to evidence from basic science, which indicates that ankle distraction leads to cartilage repair, decreased inflammation, bone density changes, and the production of a layer of slime in the joint. It has also been shown to produce periarticular osteopenia, which has been hypothesized to reduce the impact on cartilage repair through increased stress absorption by less dense bone. Dr Beaman suggested that ankle distraction can be useful on a case-by-case basis. Patients with periarticular deformity and arthritis, chondrolysis, osteochondral defects, ankle contractures, instability, and hindfoot-motion loss are good candidates. Contraindications include infection, vascular disease, neuropathy, neuroarthropathy, ankyloses, and loss of ankle-motion functions.
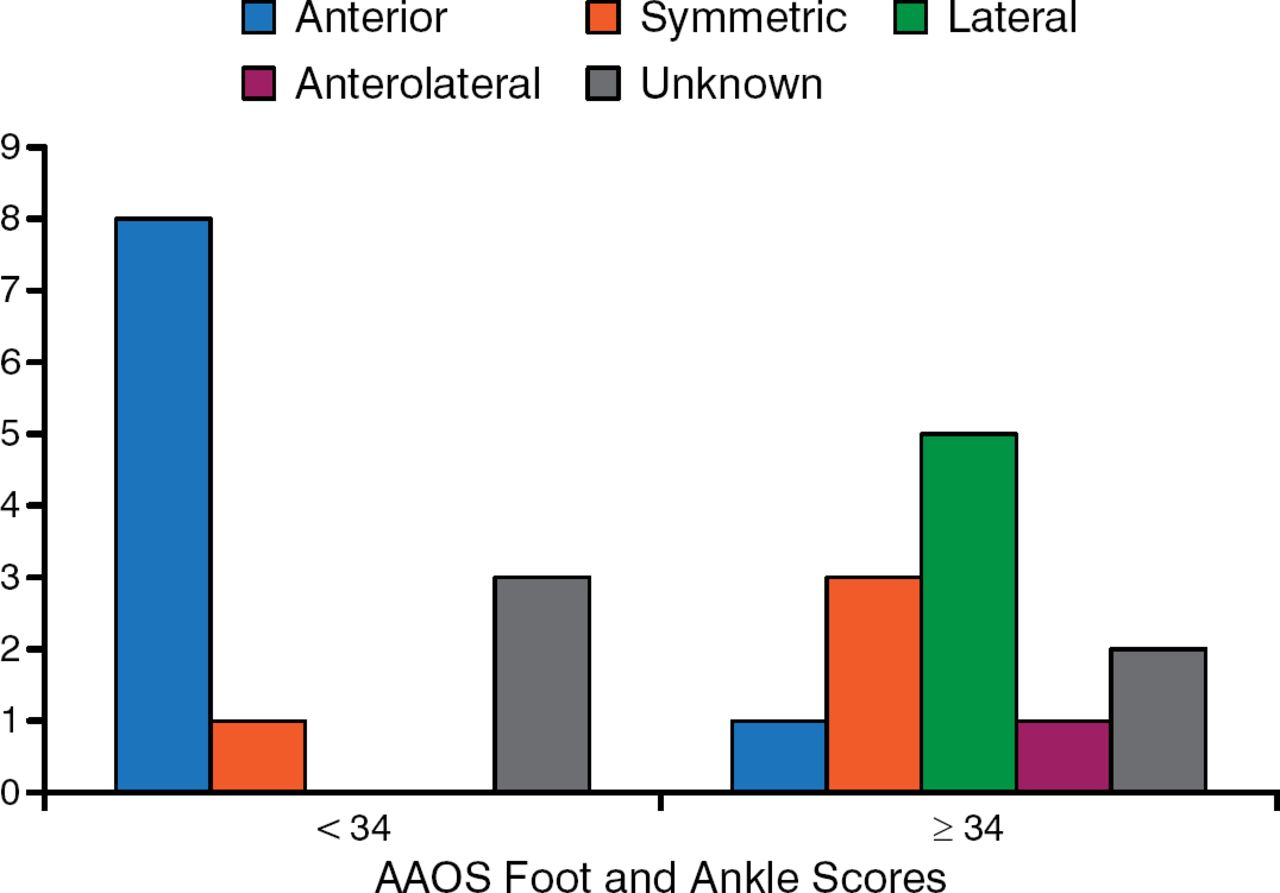
Results for joint distraction have been mixed. Results of a recent multicenter review of 105 patients showed a 44% failure rate over 12 years (17% within 2 years and 37% within 5 years) [Marijnissen AC et al. J Orthop Res. 2014]. Female sex and baseline pain levels were predictive for failure after 2 years. Patients do better with dorsiflexion, which directly correlates with the American Academy of Orthopaedic Surgeons (AAOS) score. Patients do worse with anterior joint wear, which is directly correlated to a poor AAOS score (Figure 1).

Anterior Joint Involvement and American Academy of Orthopaedic Surgeons Score
AAOS, American Academy of Orthopaedic Surgeons.
Reproduced with permission from DN Beaman, MD.
Although solid evidence is lacking to support the use of distraction [Smith NC et al. Foot Ankle Int. 2012], Dr Beaman would consider its use for a mobile joint without incongruent anterior wear for patients with a reasonable level of preoperative pain who have a clear understanding of the procedure, reasonable expectations, and patience.
Ankle fusion is a reliable, low-risk procedure that offers considerable pain relief, but is often considered a salvage and undesirable procedure, according to Judith F. Baumhauer, MD, MPH, University of Rochester Medical Center, Rochester, New York, USA. Dr Baumhauer believes that ankle fusion can relieve pain and improve function despite the loss of ankle motion if the right approach and preparation are used in the right patient.
Indications include end-stage ankle arthritis, salvage or failed total ankle replacement, acute severely comminuted unreconstructable pilon fracture, and unsalvageable ankle malalignment. Patients with isolated ankle joint arthritis, or slop or good accessory motion in the midfoot, and individuals whose occupation requires heavy use of the ankle (eg, laborers) are good candidates. Patients who smoke or who have poorly controlled diabetes, poor blood supply to the foot, or adjacent joint arthritis are poor candidates and are at higher risk for complications. Approaches include external fixation, arthroscopic/mini-open, and open (lateral, anterior, or posterior) techniques.
When performing ankle fusions, surgeons should avoid excessive soft-tissue stripping to improve healing and subsequently remove osteophytes, denude the cartilage, and perform subchondral bone perforation (drilling), while avoiding excessive heat in this preparation [Bertollo N, Walsh WR. Drilling of bone: Practicality, limitations and complications associated with surgical drill-bits. In: Klika V, ed. Biomechanics in Applications. In Tech. 2011]. According to Dr Baumhauer, the goal is a plantigrade foot with excellent bone contact; if needed, bone grafting should be considered, especially in patients aged > 50 years. The device used for stability (crossed compression screws, plates, screws, etc) should be tailored to the bone quality and patient.
For postoperative care, Dr Baumhauer recommended that patients remain casted nonweightbearing for 6 weeks and in a walking cast for a subsequent 6 weeks and that they participate in formalized or home physical therapy for 6 weeks. Possible complications include infection, wound healing problems, non- or malunion, adjacent joint arthritis or pain, nerve injury, and tibia stress fractures. Functional improvements as high as 70% to 85% have been reported, as well as 80% to 90% for relief of pain [Hendrickx RP et al. Foot Ankle Int. 2011; Zwipp H et al. Clin Orthop Relat Res. 2010; Kennedy JG et al. Clin Orthop Relat Res. 2006].
End-stage ankle arthrosis is one of the leading causes of chronic disability in North America and its severity can equal that of end-stage hip arthrosis [Glazebrook M et al. J Bone Joint Surg Am. 2008]. Sheldon S. Lin, MD, Rutgers New Jersey Medical School, Newark, New Jersey, USA, discussed the pharmacological options for treating ankle osteoarthritis (OA).
Mild OA can be treated with exercise, physical therapy, weight loss, orthotics, and nutraceuticals (ie, glucosamine, chondroitin sulfate). Surgery is usually reserved for severe cases. Moderate OA is usually treated with cyclooxygenase-2 inhibitors, high-dose nonsteroidal anti-inflammatory drugs (NSAIDs), or steroids; however, there are few studies to justify the use of these treatment strategies.
Compounding this, NSAIDs cause hypertension and upper gastrointestinal events [Laine L. Gastroenterology. 2001] and can result in hospitalization or death because of toxicity in some cases. Although steroid injections relieve pain, they can also increase hepatic glucose synthesis [Cole BJ, Schumacher HR Jr. J Am Acad Orthop Surg. 2005] and antagonize insulin effects causing chondrotoxicity [Farkas B et al. Clin Orthop Relat Res. 2010; Fubini SL et al. J Orthop Res. 2001]. Intra-articular steroid injections can cause tendon rupture, skin discoloration, fat thinning, and cartilage degeneration. There is a paucity of information regarding the efficacy of local steroid use for OA of the ankle. According to Dr Lin, the benefits of local intra-articular steroid injections into the ankle may only last 4 to 8 weeks and repeated injections are often needed.
Platelet-rich plasma (PRP) is a treatment for OA often used by athletes. When activated, PRPs release growth factors (platelet-derived, transforming, vascular endothelial, epidermal, and insulin-like) that play an important role in bone and soft-tissue healing. There have been no studies on the effectiveness of PRP in ankle OA [Vannini F et al. Foot Ankle Surg. 2014].
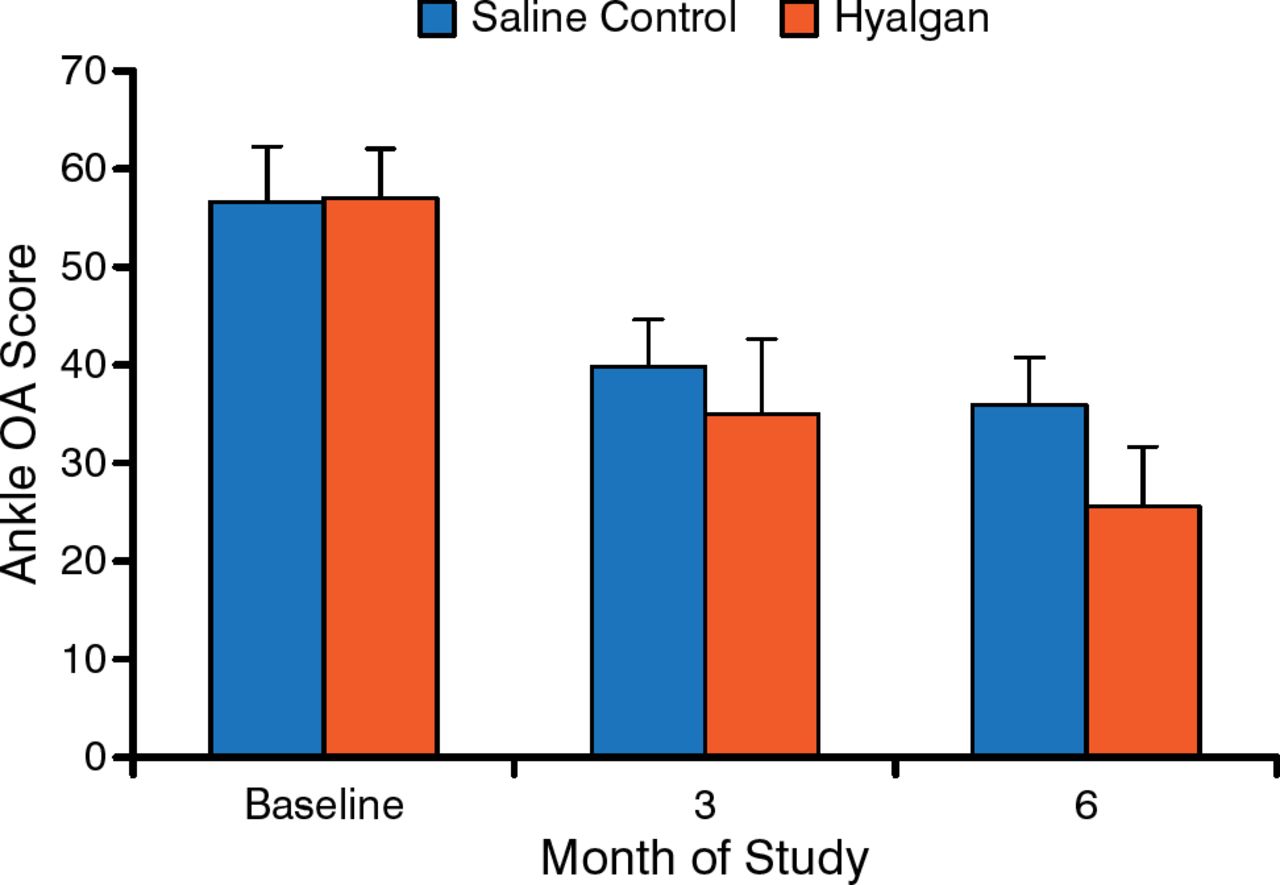
Hyaluronic acid (HA) is derived from rooster combs and was first approved for treatment of knee OA in 1997; it is not approved for ankle OA. HA protects cells, tissues, and pain receptors, thereby reducing pain during normal movement. Tang and colleagues [Arthritis Res Ther. 2008] showed that HA treatment suppressed morphological progression of OA in a strenuous-running animal model. In humans with ankle OA, 5 weekly intra-articular injections of sodium hyaluronate provided sustained relief of pain and improved function [Salk RS et al. J Bone Joint Surg Am. 2006]. In this study, although Short Form-12 health survey scores for physical function and limitation, and pain and vitality improved more for sodium hyaluronate compared with the saline control group at 6 months, both groups showed significant improvement in mean ankle OA scores at all follow-up visits from 1 to 6 months (P < .0001; Figure 2).

Mean Ankle Osteoarthritis Scores Between Sodium Hyaluronate and Saline
OA, osteoarthritis.
Reproduced from Salk RS et al. Sodium hyaluronate in the treatment of osteoarthritis of the ankle: A controlled, randomized, double-blind pilot study. J Bone Joint Surg Am. 2006;88:295–302. With permission from The Journal of Bone and Joint Surgery Inc.
One study showed HA to be effective in relieving pain associated with ankle OA at 3 months but not at 6 months [Cohen MM et al. Foot Ankle Int. 2008], whereas another study reported no difference between HA and saline injection [DeGroot H 3rd et al. J Bone Joint Surg Am. 2012]. Additional and larger studies are needed to clarify the discrepancies in these findings.

The editors would like to thank the many members of the 2014 International Federation of Foot & Ankle Societies and the American Orthopaedic Foot & Ankle Society presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.