

Summary
Surgical interspinous implants have been used to treat intermittent neurogenic claudication in patients with lumbar spinal stenosis. Some evidence has suggested it provided better outcomes compared with no (conservative) treatment. This article presents the 2-year results of the Surgical Interspinous Implant versus Conventional Decompression for Lumbar Spinal Stenosis trial that compared surgical interspinous implants to conventional decompression for patients with 1- or 2-level lumbar spinal stenosis.
- Spine Conditions
- Orthopaedics Clinical Trials
- Orthopaedic Procedures
- Spine Conditions
- Orthopaedics Clinical Trials
- Orthopaedics
- Orthopaedic Procedures
Surgical interspinous implants have been used to treat intermittent neurogenic claudication in patients with lumbar spinal stenosis. Some evidence has suggested it provided better outcomes compared with no (conservative) treatment [Moojen WA et al. Eur Spine J. 2011]. In 2011, > 30% of spine centers used implants [Overdevest GM et al. Acta Neurochir (Wien). 2014]. However, no clinical trial has been conducted to compare the efficacy of surgical interspinous implants with the gold-standard spinal bony compression.
Wouter A. Moojen, MD, PhD, MSc, Leiden University Medical Center, Leiden, The Netherlands, presented the 2-year results of the Surgical Interspinous Implant versus Conventional Decompression for Lumbar Spinal Stenosis trial [Moojen W et al. Spine. 2014] that compared surgical interspinous implants to conventional decompression for patients with 1- or 2-level lumbar spinal stenosis.
In this multicenter controlled, double-blinded trial, Moojen and colleagues randomized 159 patients with 1-or 2-level lumbar spinal stenosis for whom conservative treatment had failed to interspinous implant (n = 80) or bony decompression (n = 79).
The baseline characteristics, incision size, and postoperative care were similar in both groups. Surgery was performed on 2 levels in 18% of patients in the decompression group and 26% in the implant group. The visual analog scale (VAS) leg-pain score was between 52 and 58, and the VAS back pain score was between 60 and 49.
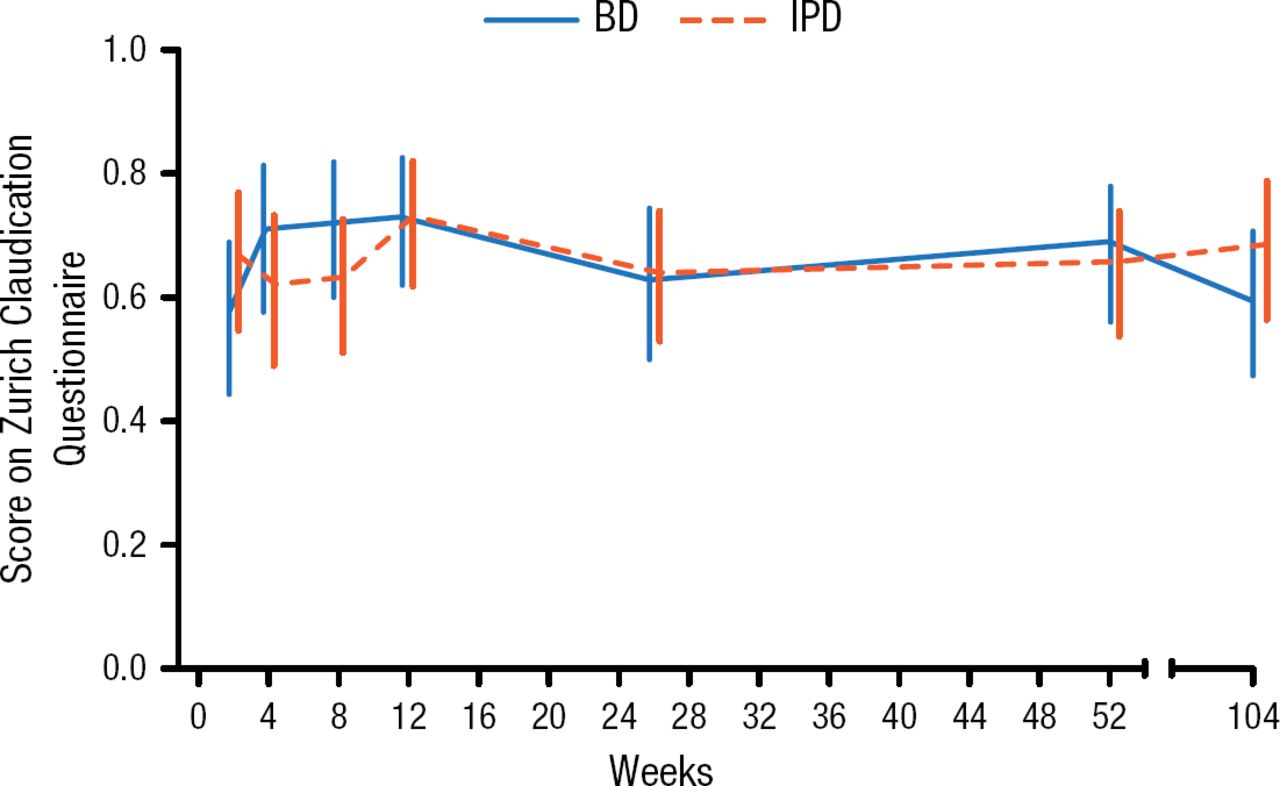
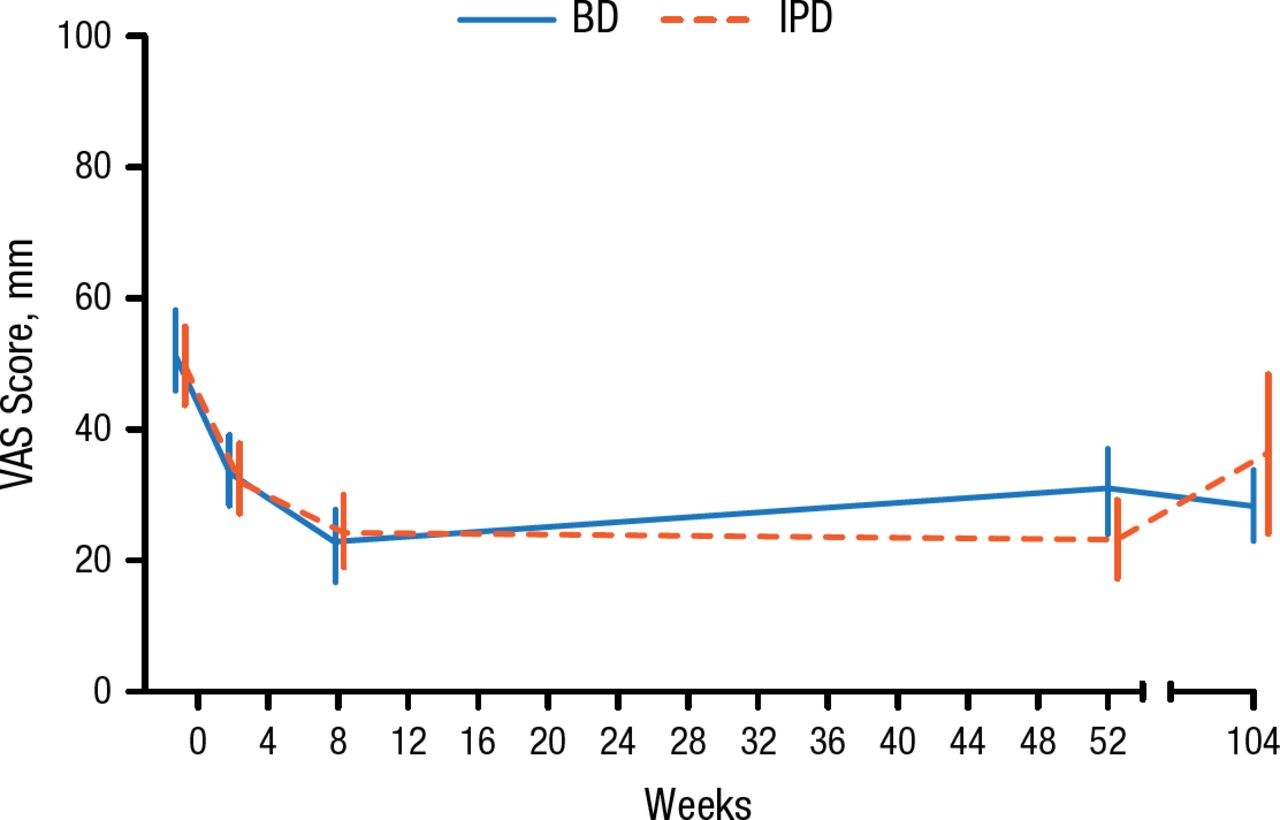
The investigators evaluated symptom severity, physical function, and patient satisfaction at 8 weeks using the Zurich Claudication Questionnaire and found no difference between the 2 groups at 1 year or 2 years (Figure 1). Further, no difference was found between the 2 groups at 8 weeks, 1 year, or 2 years for back pain as measured with the VAS score (Figure 2). The analyses were intention-to-treat.

Zurich Claudication Questionnaire Results
BD, bony decompression; IPD, interspinous process distraction. Reproduced with permission from WA Moojen, MD.

VAS Back Pain Results
BD, bony decompression; IPD, interspinous process distraction; VAS, visual analog scale. Reproduced with permission from WA Moojen, MD.
For patients treated with implants, the study found a significantly higher rate of re-operations compared with the bony decompression group (33% vs 8%; P value not reported). The rate of successful recovery after re-operation was lower than after the first operation.
In summary, this study found that clinical outcomes were similar with surgical interspinous implants and conventional bony decompression at 2 years. Back pain, as measured by the VAS score, was not reduced with surgical interspinous implants. Further, it was associated with the need for additional surgery.
Prof Moojen stated that similar results were obtained in other clinical trials of implants in this setting [Davis RJ. Spine. 2013; Strömqvist BH. Spine (Phila Pa 1976). 2013; Richter A. Eur Spine J. 2010]. Taken together with the data from the present study, Prof Moojen concluded that surgical interspinous implant confers no advantage over conventional bony decompression in patients with lumbar spinal stenosis. Conventional decompression should remain the standard for treatment.
- © 2015 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.