

Summary
Weight loss in patients with atrial fibrillation and a body mass index > 27 kg/m is associated with dose-dependent improved control of sinus rhythm and lower atrial fibrillation burden, according to the 5-year LEGACY study. However, > 5% weight fluctuation can offset these benefits.
- obesity
- atrial fibrillation
- antiarrhythmic drugs
- ablation
- weight loss
- LEGACY
- ACTRN12614001123639
- cardiology & cardiovascular medicine clinical trials
- arrhythmias
- cardiometabolic disorder
Steady, sustained weight loss can help control atrial fibrillation (AF) in overweight patients, even freeing some from the need for medications or surgical ablation. Rajeev K. Pathak, MBBS, University of Adelaide and Royal Adelaide Hospital, Adelaide, Australia, presented findings from the 5-year LEGACY trial [Pathak RK et al. J Am Coll Cardiol. 2015].
The incidence of AF is increasing in concert with the global increase in the body mass index (BMI), perhaps in part because of the influence of shared risk factors for the metabolic syndrome, as suggested by the ARIC cohort study [Chamberlain AM et al. Am Heart J. 2010]. In 2013, a smaller, 15-month study on short-term weight loss and metabolic risk factor management found reductions in AF symptoms and severity after a weight management intervention [Abed HS et al. JAMA. 2013].
LEGACY investigators enrolled 355 patients with AF and a BMI ≥ 27 kg/m2 who agreed to participate in a physician-led metabolic risk factor and weight management clinic. The study sought to determine whether there was a dose-dependent relationship between long-term weight loss and freedom from AF and the impact of fluctuations in weight on AF.
The co-primary outcomes were AF symptom burden measured by a validated questionnaire and freedom from AF by 7-day Holter monitoring. Secondary outcomes were the impact of weight loss on left atrial volume and left ventricular (LV) thickness, and metabolic and inflammatory risk factors.
After participating in the clinic, patients were divided into 3 groups: group 1, > 10% weight loss (WL; n = 135); group 2, 3% to 9% WL (n = 103); and group 3, < 3% WL, or weight gain (n = 117).
Baseline characteristics, including age, BMI range, metabolic syndrome risk factors, coronary artery disease, and sleep apnea incidence, were similar across the groups. Annual follow-up determined changes in weight.
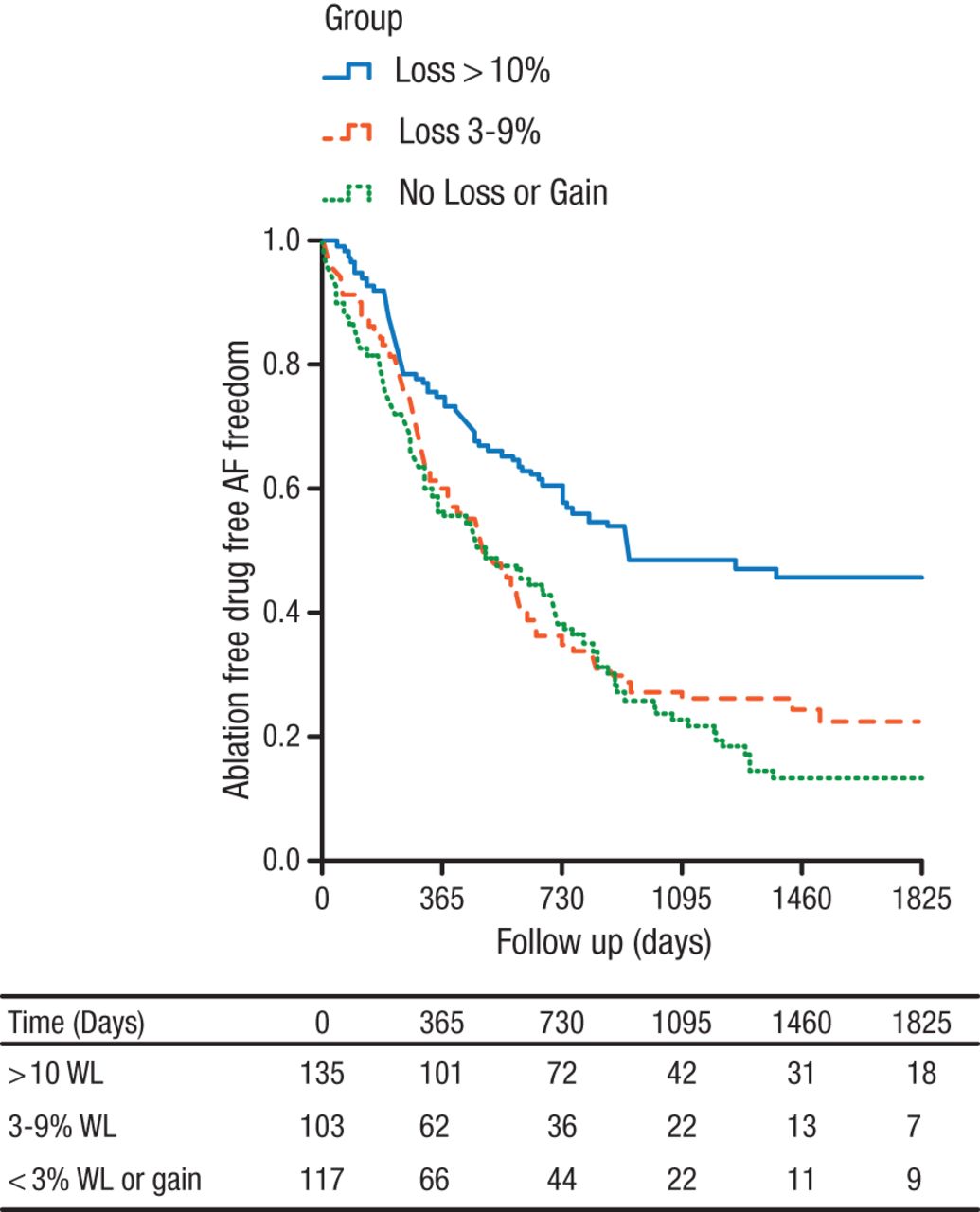
A dose-dependent relationship between weight loss and risk factors for the metabolic syndrome was found. Stepwise reductions in AF frequency, severity, and duration were found, along with stepwise increases in global well-being scores. This was most marked in group 1, in which nearly half of patients had freedom from AF without medications or ablation (Figure 1). Total arrhythmia-free survival was 86% in group 1, 66% in group 2, and 40% in group 3 (P < .001).
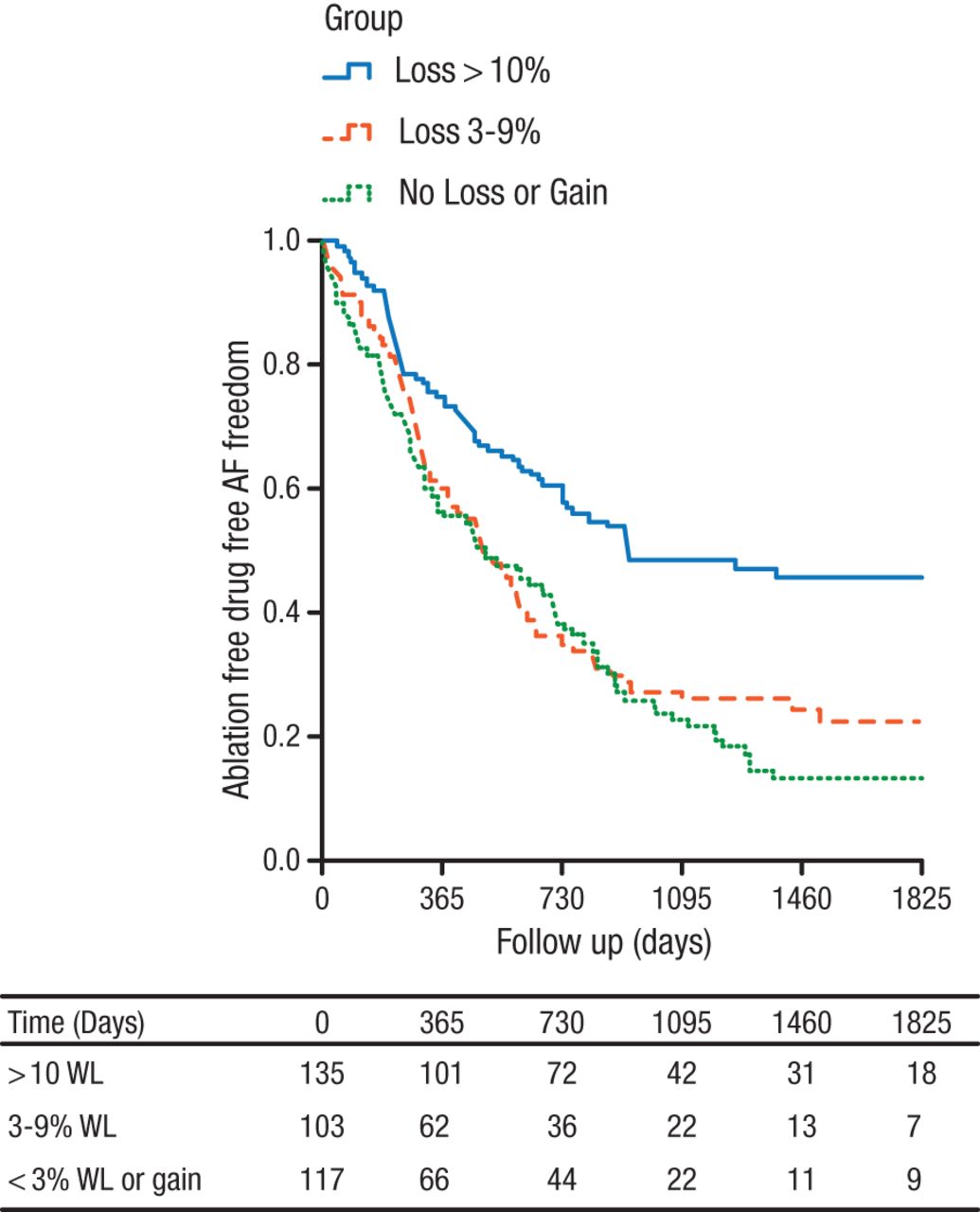
Freedom From Antiarrhythmic Drugs, Ablation, and Atrial Fibrillation
AF, atrial fibrillation; WL, weight loss.
Reprinted from J Am Coll Cardiol, Pathak RK et al. Long-term effect of goal directed weight management in an atrial fibrillation cohort: a long-term follow-up study (LEGACY Study). Article in Press, DOI: 10.1016/j.jacc.2015.03.002. Copyright (2015), with permission from American College of Cardiology.
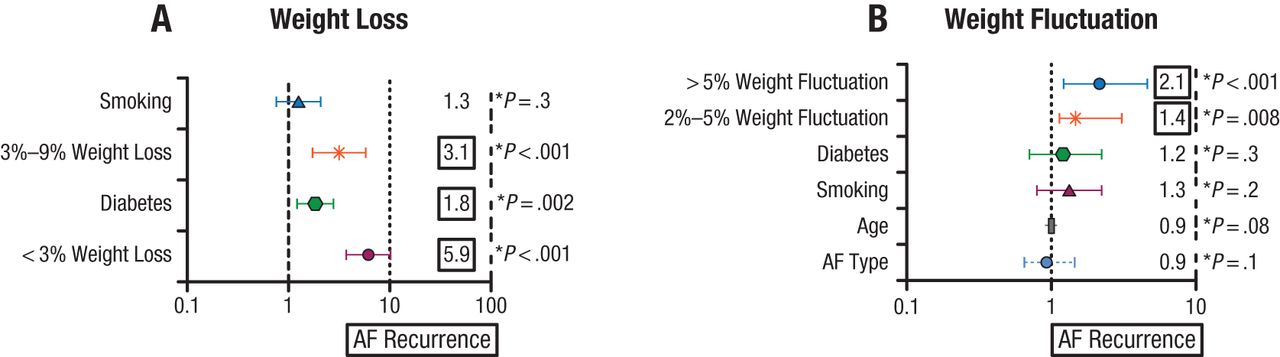
According to the multivariate analysis, a greater weight loss was associated with greater AF-free survival, while greater fluctuations in weight were associated with AF recurrence (Figure 2).
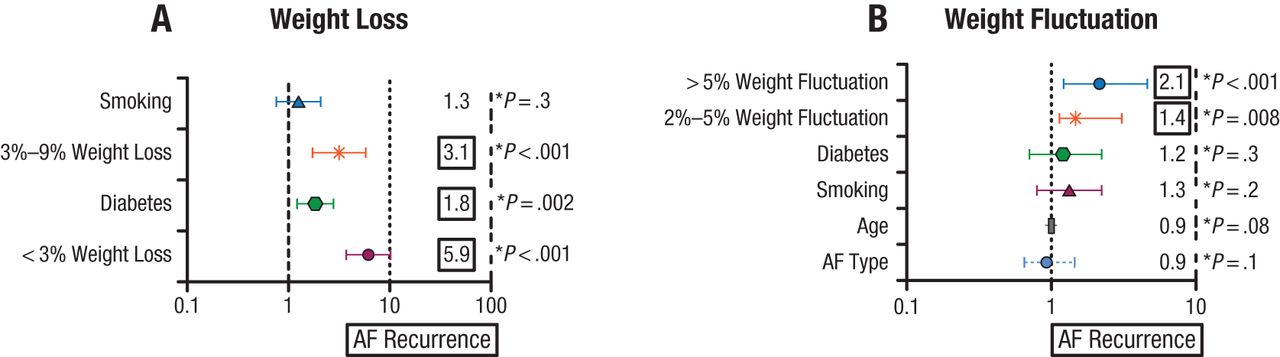
Multivariate Predictors of Atrial Fibrillation-Free Survival and Atrial Fibrillation Recurrence
AF, atrial fibrillation.
(A) ≥ 10% weight loss was associated with AF-free survival (HR, 5.7; 95% CI, 3.3 to 10.1; P < .001).
(B) > 5% weight fluctuation was associated with AF recurrence (HR, 2.2; 95% CI, 1.1 to 4.2; P < .001).
Reproduced with permission from RK Pathak, MBBS.
Source: Pathak RK et al. J Am Coll Cardiol. 2015.
In regard to structural remodeling, there were greater reductions in left atrial volume and LV thickness as compared with baseline with more weight loss.
The LEGACY trial showed that sustained weight loss in obese patients appeared to improve AF burden and heart rhythm control, although weight fluctuations of > 5% reduced this benefit. The study also showed that a dedicated weight loss clinic improved patient engagement, promoted treatment adherence, and prevented regaining weight and weight fluctuations.
- © 2015 SAGE Publications
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.