

Summary
The session “Sleep for the Practicing Neurologist” includes a presentation on the challenges of diagnosis and treatment for hypersomnolence disorders, including idiopathic hypersomnia and narcolepsy with and without cataplexy. The second presentation focuses on the association between obstructive sleep apnea and increased incidence of cardiovascular events, particularly stroke.
- cardiovascular events
- cataplexy
- death
- hypersomnia
- hypersomnolence
- International Classification of Sleep Disorders
- obstructive sleep apnea
- stroke
- narcolepsy type 1
- type 2
- neurology clinical trials
- episodic & paroxysmal disorders
In a session designed to investigate various sleep orders, 2 speakers presented new theories and updates on topics related to hypersomnolence and obstructive sleep apnea (OSA).
Lynn Marie Trotti, MD, Emory University, Atlanta, Georgia, USA, discussed the diagnostic challenges and emerging treatments of disorders of daytime sleepiness that occur despite sufficient quality, quantity, and timing of nocturnal sleep, collectively referred to as hypersomnolence. Patients with hypersomnolence experience an excessive duration of sleep, deteriorated quality of wakefulness, and sleep inertia.
The International Classification of Sleep Disorders (ICSD) recently updated naming conventions for hypersomnolence disorders [American Academy of Sleep Medicine. ICSD, 3rd ed. 2014]. Narcolepsy with cataplexy and narcolepsy without cataplexy have been reclassified as narcolepsy types 1 (NT1) and 2 (NT2), respectively. Instead of basing the definition on the absence or presence of cataplexy, it is now based on the absence (NT1) or presence (NT2) of hypocretin measured in cerebrospinal fluid. The new classification of idiopathic hypersomnia (IH) now encompasses the formerly split classifications of IH with ≥ 10 hours sleep and IH with < 10 hours sleep.
An ideal diagnostic test for hypersomnolence disorders would be sensitive for problematic sleepiness, specific for pathologic sleepiness, and reproducible, and it would appropriately categorize patients based on phenotype. The Multiple Sleep Latency Test (MSLT) is heavily relied on to differentiate among hypersomnolence disorders. However, a study found that 71% of patients with IH and long sleep have a normal MSLT [Vernet C, Arnulf I. Sleep. 2009]. Another study reported that among 100 patients with excessive daytime sleepiness, 24-hour polysomnography results were indistinguishable between patients with IH and those with subjective excessive daytime sleepiness [Pizza F et al. J Sleep Res. 2013]. Two studies found that the MSLT had poor test-retest reliability [Goldbart A et al. Sleep. 2014; Trotti LM et al. J Clin Sleep Med. 2013].
The third edition of ICSD recommends that, in addition to a sleep log, patients should be assessed with actigraphy for 1 to 2 weeks before the MSLT [American Academy of Sleep Medicine. ICSD, 3rd ed. 2014]. In a study of drug-naïve patients with NT1 (n = 39) and IH (n = 24) and 30 healthy controls, actigraphy provided a reliable objective parameter to differentiate among hypersomnolence disorders, particularly NT1 cases [Filardi M et al. Sleep Med. 2015]. A study of the Psychomotor Vigilance Task found no correlation with the MSLT, a moderate correlation with maintenance of wakefulness tests latency (r = 0.349), and strong correlation with the driving simulation test (r = −0.521) [Thomann J et al. J Clin Sleep Med. 2014].
Modafinil is a first-line treatment for patients with narcolepsy and IH. A crossover trial of modafinil vs placebo in patients with narcolepsy (n = 13) and IH (n = 14) evaluated maintenance of wakefulness tests and real driving performance after 5 days of treatment [Philip P et al. Sleep. 2014]. When treated with modafinil vs placebo, patients made fewer inappropriate line crossings (1.1 ± 0.3 vs 2.1 ± 0.7; P < .05) and had lower standard deviation of lateral position (23.6 ± 0.6 vs 24.9 ± 0.9 cm; P = .06).
Other treatments studied for hypersomnolence include pitolisant, flumazenil, and clarithromycin (Table 1).
Studies of Treatments for Hypersomnolence Disorders
Dr Trotti concluded that more studies are needed on pharmacologic treatments for hypersomnolence but some exciting advances are emerging.
OSA is a risk factor for stroke, the fifth-leading cause of death in the United States [CDC. http://www.cdc.gov/stroke/facts.htm. Accessed May 1, 2015]. Approximately 15 million adults in the United States have OSA [Somers VK et al. J Am Coll Cardiol. 2008]. The link between OSA and stroke and the impact of treating OSA were discussed by Pablo R. Castillo, MD, Mayo Clinic, Jacksonville, Florida, USA.
Nonrapid eye movement sleep is a state of cardiovascular quiescence, with reduced sympathetic activity, heart rate, blood pressure, and arrhythmogenicity. OSA causes chronic intermittent hypoxia, nocturnal sympathetic activation, sleep loss, inflammation, and metabolic dysregulation. OSA also has been identified as a secondary cause of diurnal hypertension. The American Heart Association/American Stroke Association’s guideline on preventing ischemic stroke recommends questioning patients (and their bed partners) with abdominal obesity and hypertension about symptoms of OSA and referral to a sleep specialist [Goldstein LB et al. Circulation. 2006]. The gold standard for diagnosis of OSA is attended overnight level 1 polysomnography. Other assessments include the subjective parameters of sleepiness, witnessed apneas, and snoring; morphometric data, including body mass index, neck size, and cephalometric measures; associated hypertension; and oximetry data.
About 25% of strokes occur during sleep, while wake-up stroke occurs close to awakening [Rimmele DL, Thomalla G. Front Neurol. 2014]. OSA has been shown to increase the risk of stroke independent of traditional risk factors, such as hypertension and diabetes [Mohsenin V. Am J Med. 2015]. In a 2005 study of 1022 consecutive patients with no previous stroke, 68% had OSA. The probability of event-free survival was significantly lower for patients with OSA compared with controls (log-rank P = .003). Trend analysis showed a stepwise increase in the risk of stroke or death with increasing OSA severity (P = .005; Table 2). A significant association was found between OSA and stroke or death from any cause in unadjusted (HR, 2.24; 95% CI, 1.30 to 3.86; P = .004) and adjusted analyses (HR, 1.97; 95% CI, 1.12 to 3.48; P = .01).
Trend Analysis for Relationship Between Increased OSA Severity and Composite of Stroke or Death From any Cause
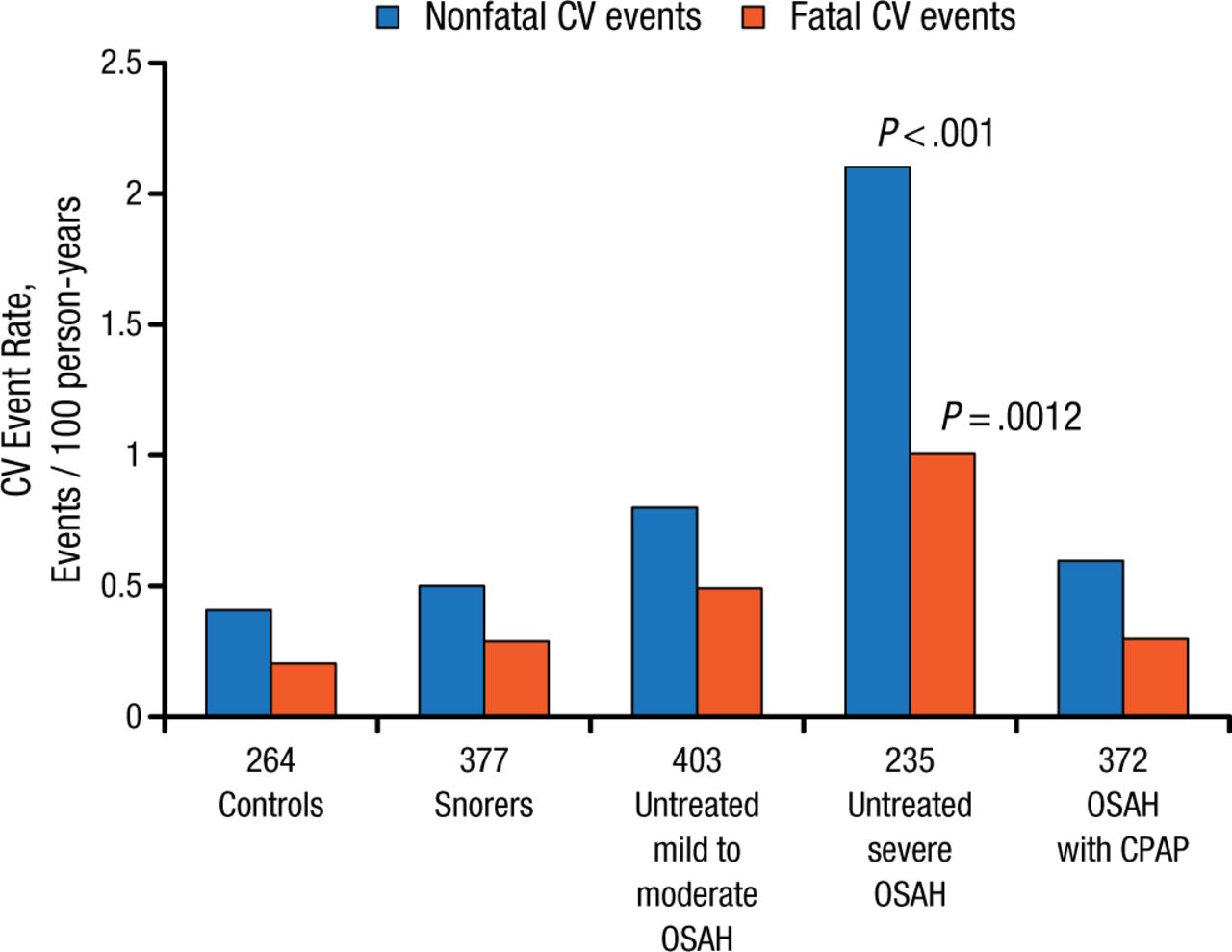
Treatment of OSA was associated with better cardiovascular outcomes before treatment with continuous positive airway pressure (CPAP) became available. In a 2005 study, the potential protective effect of CPAP was studied in a male population of 264 healthy men, 377 simple snorers, 403 with untreated mild to moderate OSA, 235 with untreated severe OSA, and 372 with CPAP-treated OSA. Patients with untreated severe OSA had a significantly higher incidence of fatal (1.06/100 person-years) and nonfatal (2.13/100 person-years) cardiovascular events compared with the other groups (Figure 1).

Incidence of Fatal and Nonfatal CV Events
CV, cardiovascular; CPAP, continuous positive airway pressure; OSAH, obstructive sleep apnea-hypopnea syndrome.
Source: Marin JM et al. Lancet. 2005.
Reproduced with permission from PR Castillo, MD.
OSA is a valid syndrome that increases cardiovascular risk. The long-term ongoing randomized SAVE trial [NCT00738179] is examining whether CPAP treatment of OSA reduces the risk of cardiovascular events. The trial has a global recruitment target of 5000 patients, and results are expected in early 2016.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.