

Summary
Addenbrooke's Hospital in Cambridge, United Kingdom, once known for having high rates of Staphylococcus aureus bloodstream infections, has been able to significantly reduce rates of methicillin-susceptible S. aureus and methicillin-resistant S. aureus BSIs using a number of infection control interventions.
- Screening & Prevention
- Bacterial Infections Clinical Trials
Addenbrooke's Hospital in Cambridge, United Kingdom, once known for having high rates of Staphylococcus aureus bloodstream infections (BSIs), has been able to significantly reduce rates of methicillin-susceptible S. aureus (MSSA) and methicillin-resistant S. aureus (MRSA) BSIs using a number of infection control interventions under the lead of Infection Control Doctor Nick Brown, MD. Staff physician Theodore Gouliouris, MD, presented data from a study that showed a decline in MRSA and MSSA BSI rates that was driven by reductions in nosocomial infections.
The purpose of the study was to analyze trends of MSSA and MRSA BSIs according to onset (community vs hospital) and assess the impact of infection control interventions. The interventions were initiated over several years and included: starting a hand hygiene campaign (November 2004), establishing a vascular access team (January 2006), improving line care bundles (June 2006), screening all emergency (April 2007) and elective (January 2009) admissions for MRSA carriage, and routinely decolonizing all MRSA-positive patients (entire study period). This was a retrospective study in a tertiary referral university hospital setting with 1200 beds and 70,000 in-patient admissions per year. All S. aureus bacteremia (SAB) episodes from January 2001 to December 2010 at Addenbrooke's Hospital were included. The number of episodes was converted to rates per 1000 bed days, which allowed comparison with other hospitals. Only the first episode of SAB per patient during the study period was analyzed. Patients were categorized according to onset: community onset (<48 hours from hospital admission) and nosocomial onset (≥48 hours from hospital admission).
There were 1607 SAB episodes following deduplication; 861 (53.6%) MSSA, of which 437 (50.8%) were community onset and 424 (49.2%) were nosocomial onset, and 746 (46.4%) MRSA, of which 163 (21.8%) were community onset and 583 (78.2%) were nosocomial onset.
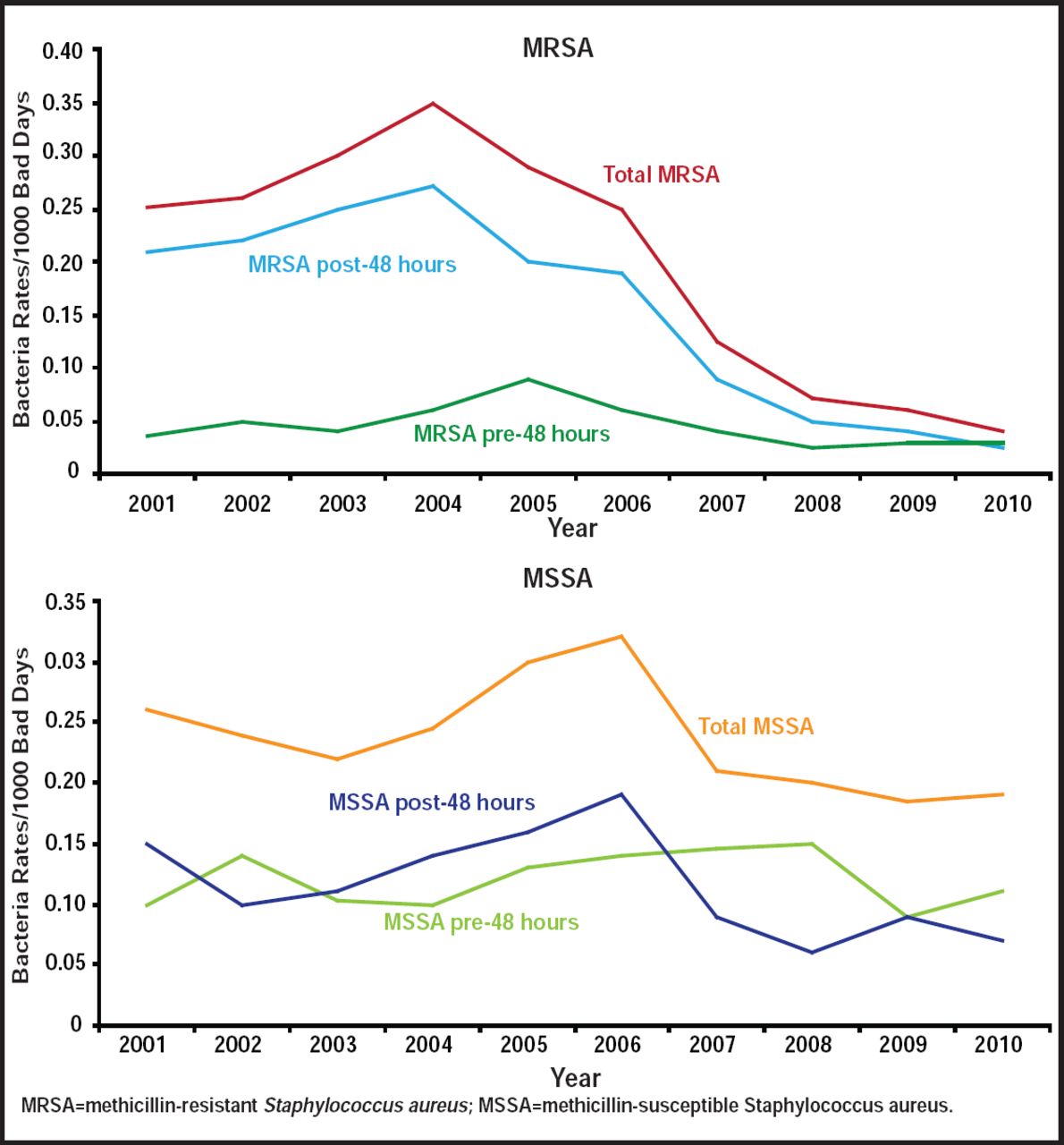
MRSA rates started to decline in 2004, driven more by a reduction in nosocomial infections, with the largest decrease (53%) occurring during the 2006 to 2007 period. MSSA rates started to decline in 2006, driven again by reductions in nosocomial infections, with the largest decrease (59%) occurring during 2006–2007. Community-acquired infections remained stable over the same period (Figure 1). Hand washing affected MRSA transiently but not MSSA rates, while having a vascular access team and performing line care bundle had a large impact on decreases for both MRSA and MSSA. Extended MRSA screening may have contributed to the larger decline in MRSA infections. Potential confounders (hospital 1000 bed-day activity and number of blood cultures processed) did not influence results.

Community Acquired Infection Rates.
Reproduced with permission from T. Gouliouris, MD.
The results of this study are limited by the fact that it was a retrospective, noncomparative study. There was also a lack of data regarding the MSSA molecular epidemiology in the hospital, the proportion of community-onset bacteremias that were health care-associated, and the proportion of nosocomial bacteremias that were line-related.
Dr. Gouliouris concluded from the study that local rates of nosocomial MSSA BSIs have declined since 2006, though not as markedly as those for MRSA. The establishment of a vascular access team and the implementation of line care bundles appear to have had the most impact toward reducing both nosocomial MRSA and MSSA BSIs. MRSA screening and decolonization likely accounted for the greater reductions that were achieved in MRSA BSIs compared with MSSA. Finally, MSSA-targeted interventions may be needed to achieve reductions that are comparable with those for MRSA BSIs.
- © 2011 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.