

Summary
In the VIDOS study, treatment of vitamin D–deficient postmenopausal women with vitamin D supplementation did not reduce the incidence of falls or improve physical performance. However, women who received 1600 to 3200 IU per day experienced a lower incidence of falls vs women who received placebo or lower or higher doses.
- vitamin D
- falls
- physical performance
- VIDOS study
- endocrinology, diabetes & metabolism clinical trials
Elderly women who received 1600 to 3200 IU QD of vitamin D supplementation experienced a lower incidence of falls compared with women who received lower or higher doses of vitamin D or placebo, but overall differences were not significant. Shervin Yousefian, MD, Creighton University, Omaha, Nebraska, USA, presented data from the VIDOS study [NCT00472823].
Results regarding the effect of vitamin D supplementation on falls and physical performance in elderly patients have been inconsistent. The purpose of VIDOS was to evaluate the effect of vitamin D supplementation on falls and physical performance in vitamin D–deficient postmenopausal women living in the community.
In this interventional study, 163 postmenopausal white women were randomly assigned to receive vitamin D supplementation with 400, 800, 1600, 2400, 3200, 4000, or 4800 IU QD or placebo for one year. Women were required to be vitamin D deficient, with a serum 25-hydroxyvitamin D (25[OH]D) level of ≤ 20 ng/mL. The mean age of the 147 women who completed the study was 66.2 years and the mean body mass index was 30.3 kg/m2. Patients were excluded if they had active nephrolithiasis, chronic kidney or liver disease, persistent hypercalcemia, or a medical condition prohibiting physical activity or if they had a disease or were receiving medication that affected calcium or bone metabolism. Accounting for data from 7-day food diaries, calcium supplementation was administered to achieve a daily calcium intake of 1200 mg.
In the placebo arm, patients who did not experience falls had greater serum levels of 1,25 dihydroxyvitamin D (1,25[OH]2D) than patients who did experience falls. Patients who received vitamin D supplementation demonstrated higher levels of 1,25(OH)2D compared with patients who received placebo, but there was no significant difference in 1,25(OH)2D levels between patients who did or did not experience falls, regardless of the amount of supplementation. Similarly, 25(OH)D levels increased in a dose-response fashion among patients who received supplementation; however, there was no significant difference in 25(OH)D levels between patients who did or did not experience falls.
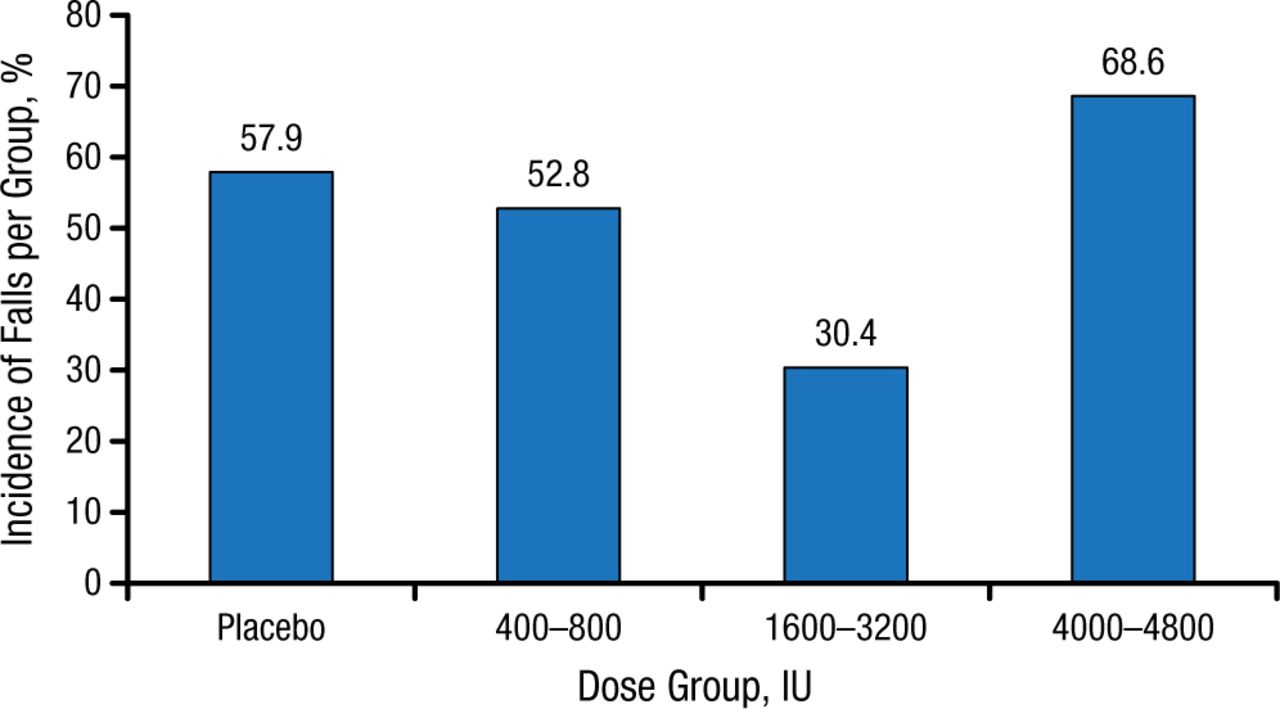
The fall rate varied among the arms of the trial. Patients in the placebo arm and those patients who received 400 to 800 IU QD of vitamin D experienced similar fall rates (Figure 1). However, the fall rate was considerably lower in patients who received 1600 to 3200 IU QD of vitamin D, whereas patients who received the largest dose of vitamin D had an even higher fall rate.
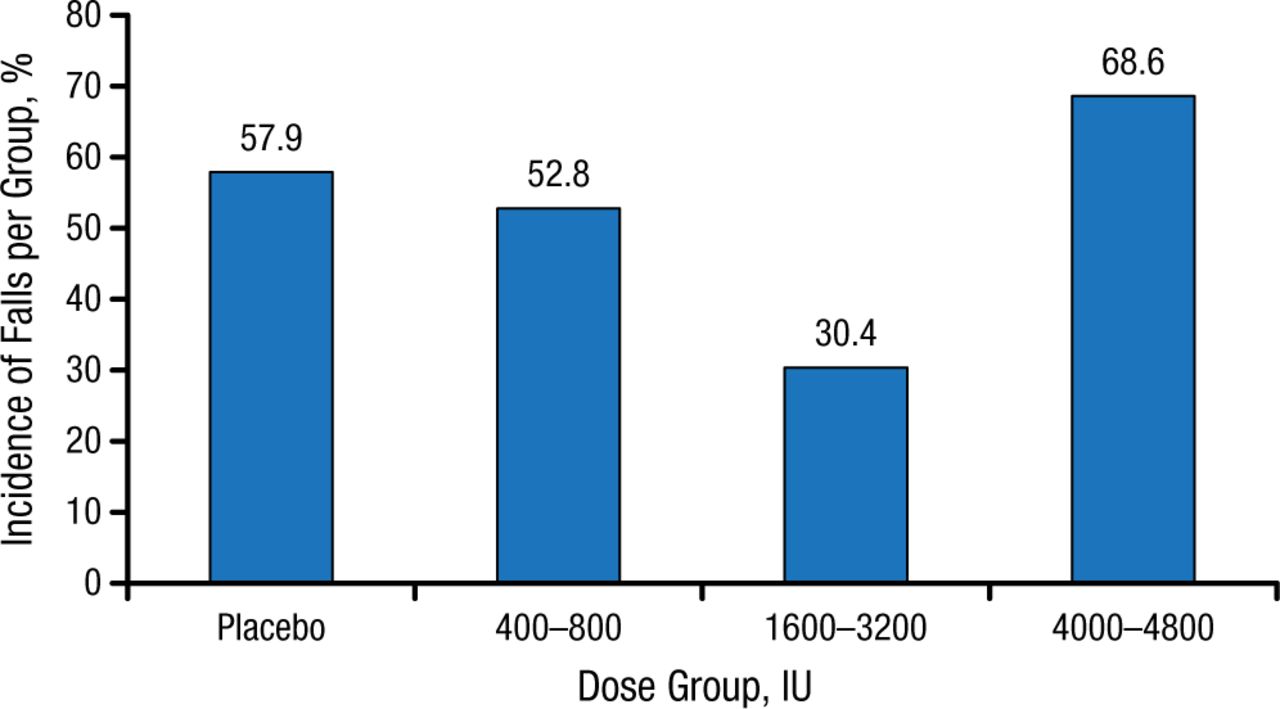
Incidence of Falls Stratified by Vitamin D Supplementation Dosage
Reproduced with permission from S Yousefian, MD.
The timed up and go (TUG) value was slower at 1 year among all arms; however, patients who received 1600 to 3200 IU QD or 4000 to 4800 IU QD of vitamin D appeared to have a slower rate of increase in the TUG value. At 1 year, there was no significant difference in the chair stand test among all of the arms.
In conclusion, the results of the VIDOS study suggest that, overall, vitamin D supplementation did not appear to improve physical performance or the incidence of falls. However, Dr Yousefian pointed out that there was a U-shaped distribution for the incidence of falls among the various doses of vitamin D supplementation, suggesting that there may be an optimal dose for fall prevention at about 2000 IU QD. However, additional larger studies are needed to better assess the role of vitamin D supplementation in the incidence of falls among elderly patients.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.