

Summary
Urinary tract infections occur at least once in up to 60% of women, with about a third of those experiencing recurrent infections. Prophylaxis with current antibiotics is effective, but can cause side effects and promote drug resistance. Novel approaches are under development that show promise in preventing and treating urinary tract infections.
- urinary tract infection
- UTI
- E coli
- bacterial infections
- infectious diseases clinical trials
- vaccinations
Up to 60% of women experience at least 1 urinary tract infection (UTI), and about one-third of those will suffer from recurrent infections. The majority of UTIs are caused by Escherichia coli, which can be sourced from multiple reservoirs, explained Marc Stegger, MSc, Statens Serum Institute, Copenhagen, Denmark.
The E coli clones found to cause most UTIs are also found in gut and fecal flora, which is related to the routes of transmission of E coli such as food animals, meat, healthy and infected people, pets, waste water, and care providers. Indeed, within the household, children, pets, and sexual partners can transmit E coli [Johnson JR et al. J Clin Microbiol. 2008].
Although food sources like meat have been previously implicated as an important reservoir for E coli–associated UTIs [Overdevest I et al. Emerg Infect Dis. 2011], more recent data from the Netherlands using whole genome sequencing have demonstrated that such transmission occurs with less frequency than originally believed [de Been M et al. PLoS Genet. 2014]. However, the US setting is different, as modern farming is predominated by concentrated animal feeding operations, which represents an ideal environment for the selection of drug-resistant bacteria. Organic farming is not immune to selection of resistant bacteria, as organic criteria allow the injection of chicken eggs with gentamicin. The question then becomes how much overlap is there between UTIs and extraintestinal pathogenic E coli (ExPEC).
To answer this question, researchers collected meat from local grocery stores in Flagstaff, Arizona (population 66 000), and E coli was sampled from bladder and kidney infections from Flagstaff Medical Center. The initial analyses using Illumina sequencing demonstrated that E coli concentrations ranged from 60% to 90% of pork, chicken, and turkey samples, whereas ExPEC levels ranged from < 10% in pork, almost 20% in chicken, and > 30% in turkey. Furthermore, antibiotic-resistant E coli was found in up to 75% of meat samples, particularly in turkey samples. Further analysis of the UTI isolates suggested that UTIs associated with E coli strain ST131 may be sourced from food; however, there was little evidence of isolate H30Rx transmission via food.
Understanding the route of transmission and potential reservoirs for E coli is important to help prevent infection or reduce practices that promote E coli habitation. In addition, Florian M.E. Wagenlehner, MD, PhD, Justus-Liebig-University, Gieβen, Germany, discussed the use of antibiotics and immunostimulation as prophylaxis for recurrent UTIs, noting that much of the relevant data is from older studies.
Low-dose antibiotics are effective in preventing recurrent UTIs in nonpregnant women. As a result of supportive evidence, the 2015 European Association of Urology guidelines recommend prophylaxis daily or after intercourse with nitrofurantoin, trimethoprim, trimethoprim-sulfamethoxazole, or fosfomycin trometamol for nonpregnant women with recurrent UTIs, and cephalexin during pregnancy [Grabe M et al. Eur Urol. 2015]. However, antibiotic prophylaxis is associated with side effects and could promote antibiotic resistance, thus contributing to future treatment failure. In a study from 2000, prophylaxis with 500 mg of ciprofloxacin was significantly associated with ciprofloxacin resistance after treatment. Therefore, Prof Wagenlehner suggested that prophylaxis be used only after behavioral modification has failed [Lichtenberger P, Hooton TM. Int J Antimicrob Agents. 2011].
An alternative to antibiotic prophylaxis is immunostimulation, such as with the oral bacterial lysate immunostimulant OM-89. Multiple placebo-controlled studies have demonstrated that the number of UTIs was substantially decreased in patients who received OM-89 compared with placebo. Indeed, a meta-analysis of 5 randomized, placebo-controlled trials of OM-89 for the prevention of UTI found that a significantly greater number of patients were free from UTIs compared with placebo (P = .001) [Naber KG et al. Int J Antimicrob Agents. 2009].
Another mechanism of prophylaxis is through vaccination against the E coli that commonly cause UTIs. Harry Mobley, PhD, University of Michigan Medical School, Ann Arbor, Michigan, USA, discussed the status of E coli vaccines. Multiple vaccine candidates have been tested [Brumbaugh AR, Mobley HL. Expert Rev Vaccines. 2012]; however, the difficulty is determining factors that differ among humans and E coli, yet are recognized by the immune system and targetable by a vaccine.
As a result of these stringent criteria, Dr Mobley stated that there are currently just 6 vaccine candidates, with outer membrane iron acquisition systems a potential target. Differential gel electrophoresis studies have demonstrated that iron receptor proteins are upregulated in the urine of patients with UTIs. Although the urinary tract is typically iron-limiting [Alteri CJ, Mobley HL. Infect Immun. 2007], iron acquisition genes appear to be induced by E coli in the host. Studies in mouse models have demonstrated that vaccines targeting heme receptors Hma and ChuA, siderophore receptor IreA, aerobactin receptor lutA [Alteri CJ et al. PLoS Pathog. 2009], and yersiniabactin receptor FyuA, as well as siderophores themselves, have reduced bacterial loads and induced an immune response when used for intranasal vaccination.
In addition, understanding how different strains of E coli adhere to the urothelial cells of the urinary tract is an important step to develop novel agents to treat UTIs. Beat Ernst, PhD, Pharmacenter University of Basel, Basel, Switzerland, discussed the pharmacokinetic requirements of such agents. Adhesion to urothelial cells is facilitated by FimH that causes pili formation, which has different affinity states depending on the bladder environment. Several antagonists to the low- and high-affinity states of pili have been in development [Kleeb S et al. J Med Chem. 2015; Scharenberg M et al. Assays Drug Dev Technol. 2011].
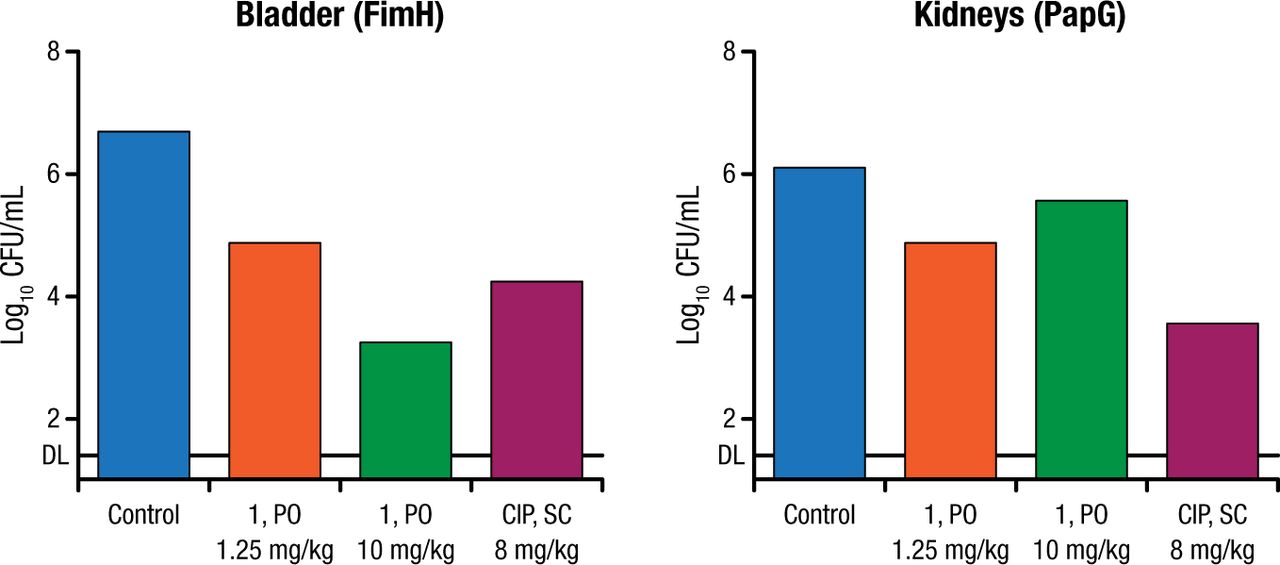
According to Prof Ernst, antagonists of pili must be selective, undergo renal excretion, have metabolic stability, be soluble, and have oral bioavailability. A recent study in a mouse model evaluated the efficacy of FimH antagonist UT189, which demonstrated decreased E coli concentration in the bladder after oral dosing and in the kidney after subcutaneous dosing (Figure 1) [Kleeb S et al. J Med Chem. 2015].

Effect of FimH Antagonist on Escherichia coli Concentration in Mice
CFU, colony forming units; CIP, ciprofloxacin; PO, orally; SC, subcutaneous.
Adapted with permission from Kleeb S et al, FimH Antagonists: Bioisosteres to Improve the in Vitro and in Vivo PK/PD Profile, J Med Chem, 2015, Vol 58, Pages 2221-2239. Copyright 2015 American Chemical Society.
In conclusion, recurrent UTIs remain a tremendous public health problem, with a large proportion of women experiencing recurrent infections. Although prophylaxis is effective for most patients with current antibiotics, this practice can lead to side effects and promotion of antibiotic resistance. Therefore, novel approaches are being developed to prevent and treat UTIs, including immunostimulation, vaccines, and targeting bacterial adhesion.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.