

Summary
Emergency department (ED) providers need to become familiar with highly infectious pathogens that may appear in patients presenting for care and should take a good travel history that includes asking about high-risk locations and exposures as well as symptom onset and duration. This article discusses ways to safely evaluate and manage patients with suspected highly infectious pathogens who present to EDs while also minimizing the safety risk to ED health care workers.
- Environmental & Wilderness Medicine
- Screening & Prevention
- Viral Infections
- Environmental & Wilderness Medicine
- Screening & Prevention
- Viral Infections
- Emergency Medicine
Emergency department (ED) providers need to become familiar with highly infectious pathogens that may appear in patients presenting for care and should take a good travel history that includes asking about high-risk locations and exposures as well as symptom onset and duration. In addition, physicians need to learn their institutional infection prevention and control guidelines and help, when needed, to update or revise existing guidelines.
David C. Pigott, MD, University of Alabama at Birmingham, Birmingham, Alabama, USA, spoke on ways to safely evaluate and manage patients with suspected highly infectious pathogens who present to EDs while also minimizing the safety risk to ED health care workers.
He focused on inhaled anthrax, plague, viral hemorrhagic fevers (Ebola and Marburg), and Middle East Respiratory-Syndrome (MERS) Coronavirus. These pathogens all meet criteria for being highly infectious: they have a significant potential for person-to-person transmission, may pose serious risk to people including health care workers in contact with the patient, are associated with a high morbidity and mortality despite treatment, and have no proven or effective therapies to treat them.
For the bulk of his presentation, Dr Pigott used case studies of patients with inhaled anthrax, plague, and the hemorrhagic fevers to walk participants through the clinical signs and symptoms, appropriate management, and follow-up for each. Table 1 illustrates one case study on a patient presenting with inhaled anthrax.
Case Study of Patient Presenting With Inhaled Anthrax
Dr Pigott emphasized that a first critical step in identifying a suspected highly infectious pathogen is to take a good travel history that can illuminate exposure, incubation period, and any vaccines or chemoprophylaxis.
The importance of getting a good travel history is highlighted by data demonstrating that about 4 million of an estimated 50 million (8%) people who travel from industrialized to developing countries each year seek medical care abroad or upon return home, and multiple reports of infectious diseases imported to industrialized countries [Freedman DO. Travel Epidemiology. Centers for Disease Control and Prevention. 2013].
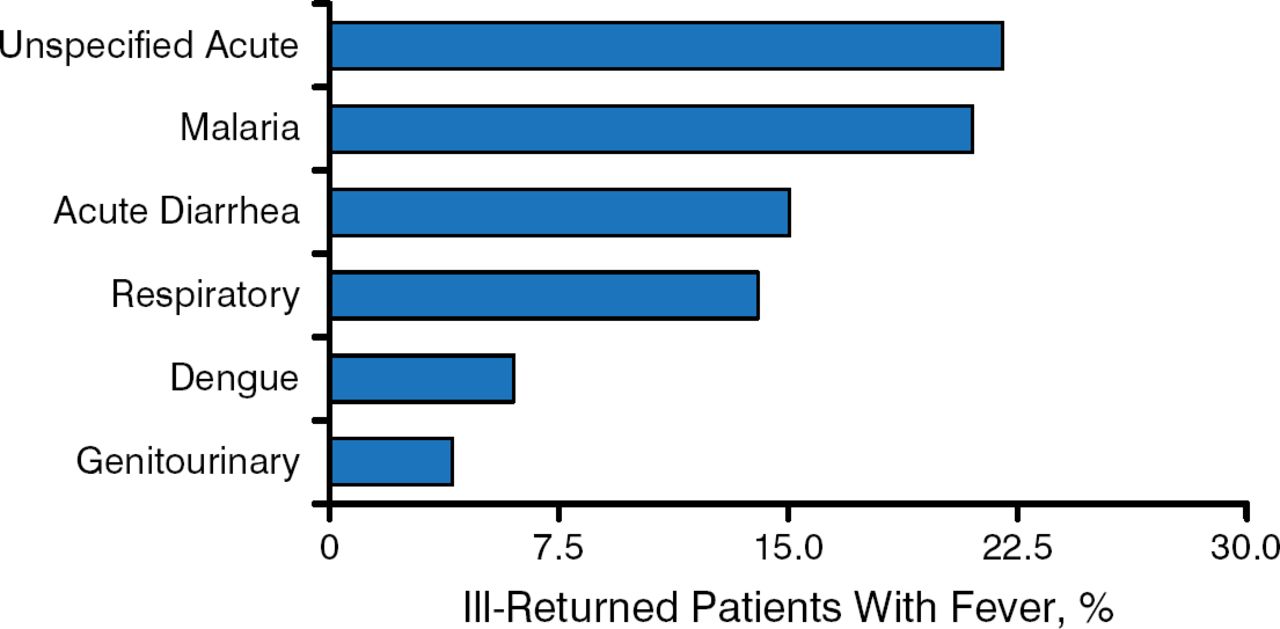
Along with taking a good travel history, emergency physicians (EPs) also need to become familiar with the clinical presentation of these pathogens, including patterns of fever and other signs and symptoms, which can help make a differential diagnosis. Data from a large study show that most febrile patients after travel present with unspecified acute symptoms (Figure 1).

Many Febrile Patients Present After Travel With Unspecified Acute Symptoms (n = 6957)
Adapted from Kotylar S et al. Fever in the returning traveler. Emerg Med Clin North Am. 2013;31:927–944. Republished with permission of Elsevier, Inc.
To conclude, physicians should become familiar with the framework for the safe evaluation of patients with suspected highly infectious pathogens in order to effectively manage patients and at the same time minimize the risk to physicians and other health care team members.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.