

Summary
The ORBIT II study demonstrates that a coronary orbital atherectomy is a potential treatment option for patients with calcified coronary lesions, with potential cost-saving benefits. Patients with diabetes treated with a coronary orbital atherectomy system have similar results to patients without diabetes.
- calcified coronary lesion
- coronary orbital atherectomy system
- economic analysis
- ORBIT II
- OAS
- PCI
- percutaneous coronary intervention
- coronary artery disease
- cardiology & cardiovascular medicine clinical trials
- interventional techniques & devices
- myocardial infarction
Jeffrey W. Chambers, MD, Metropolitan Heart and Vascular Institute, Mercy Hospital, Minneapolis, Minnesota, USA, presented 2-year results of the ORBIT II study [Généreux P et al. Am J Cardiol. 2015], demonstrating that a coronary orbital atherectomy system (OAS) can be used as a lesion preparation tool prior to stent implantation in patients with severely calcified coronary lesions, and also had potential cost-saving benefits over standard treatment.
The prevalence of risk factors for arterial calcification (eg, advanced age, diabetes, and kidney disease) is increasing rapidly in the United States. Coronary calcium is a predictor of adverse outcomes in patients undergoing percutaneous coronary intervention for acute coronary syndromes [Généreux P et al. J Am Coll Cardiol. 2014]. Diamondback 360 is the first novel coronary OAS technology approved by the FDA to specifically treat severely calcified lesions. It utilizes centrifugal sanding action, and Dr Chambers specifically highlighted its simplicity of use.
ORBIT II [Généreux P et al. Am J Cardiol. 2015] was a prospective, multicenter, nonblinded, single-arm study that evaluated the long-term safety and efficacy of coronary OAS in patients with severely calcified coronary lesions who underwent percutaneous coronary intervention. The objective of the study was to determine whether OAS successfully facilitated stent deployment and was safe in this patient population. The major inclusion criteria were evidence of severe calcification and the target vessel reference diameter between 2.5 mm and 4.0 mm, with the lesion length ≤ 40 mm.
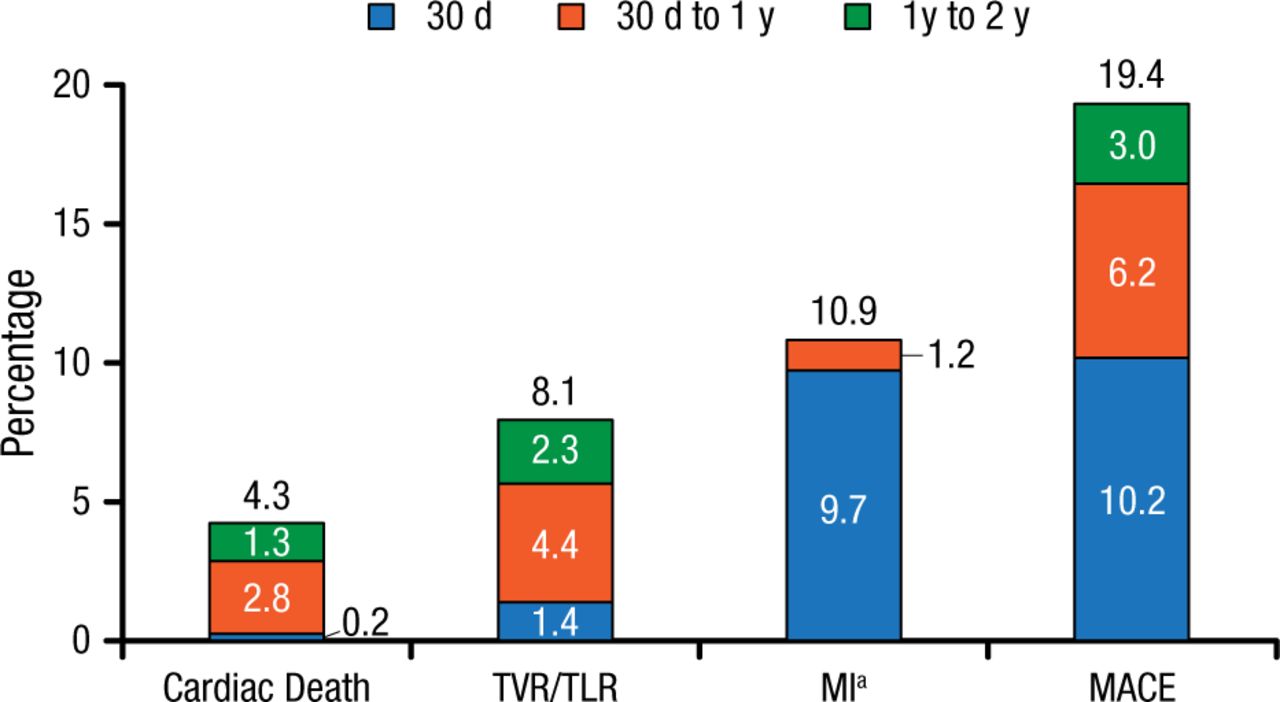
The study enrolled 443 patients (64.6% men; mean age 71.4 years), with 97.7% of patients obtaining successful stent delivery that resulted in 98.6% of patients having < 50% residual stenosis [Chambers JW et al. JACC Cardiovasc Interv. 2014]. The adjudicated safety analysis showed that at 2-year follow-up, cardiac death occurred in 4.3% of patients, target vessel revascularization (TVR)/ target lesion revascularization (TLR) in 8.1% (TLR, 6.2%; TVR, 2.9%), myocardial infarction in 10.9%, and the composite end point of major adverse cardiac events in 19.4% (Figure 1). The subanalysis of the diabetic population revealed that coronary OAS produced similar outcomes in patients with diabetes (n = 160) vs those without (n = 283) at 2-year follow-up, with major adverse cardiac events occurring in 20.6% vs 18.7%, respectively.
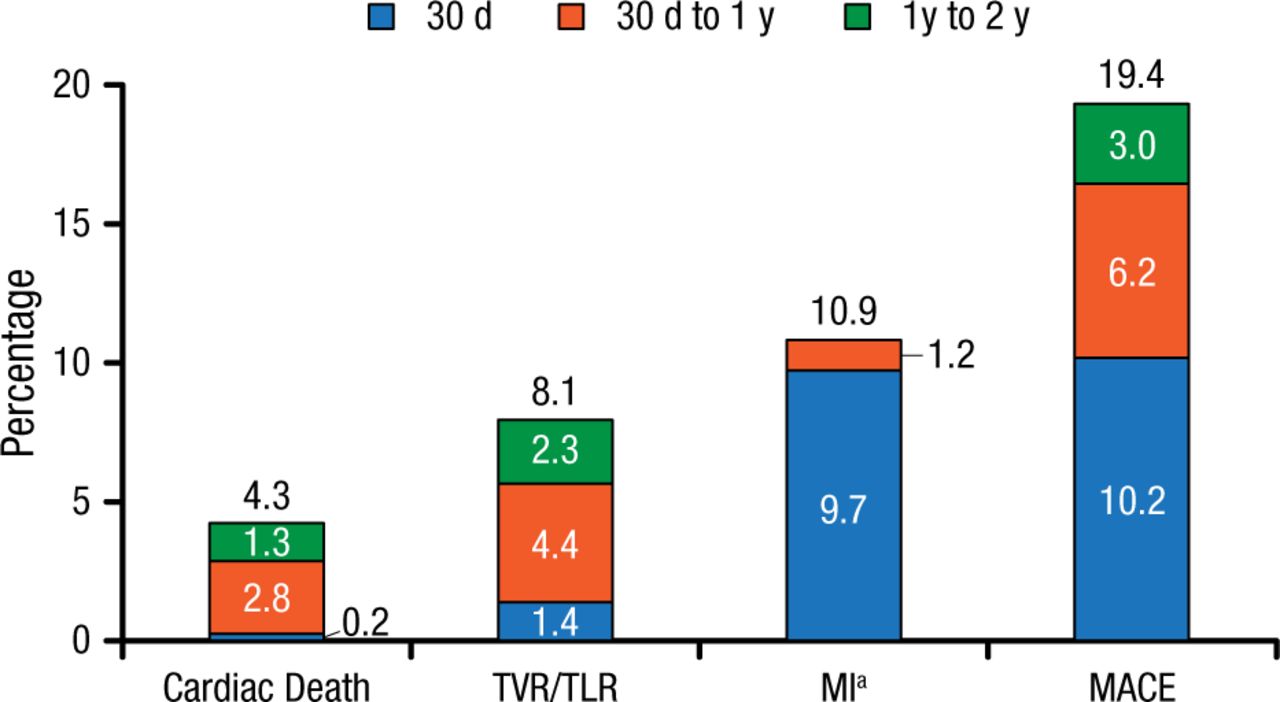
ORBIT II Safety Outcomes at 2-Year Follow-up
CEC, Clinical Events Classification; MACE, major adverse cardiac event; MI, myocardial infarction; TVR/TLR, target vessel revascularization/target lesion revascularization.
aNot per protocol analysis. Clinically driven evaluation based on CEC adjudication of MI.
Reproduced with permission from JW Chambers, MD.
The economic analysis compared OAS in elderly patients in the ORBIT II study (> 64 years; n = 297) with standard treatment in Medicare patients (n = 308) from hospitals reporting more than 10% of stent patients with calcification during the same time period. The baseline characteristics were comparable between these patient populations. The cost-model framework analysis revealed that the average projected cost offsets in the first year would fully cover the cost of OAS at $3795 and possibly extend to an additional $1118 in savings, yielding a total of $4913 in potential cost offset at 1 year. The incremental cost-effectiveness ratio (ICER) analysis demonstrated that OAS offered good value, with an ICER of $11 895 per life-year gained, which was substantially below the “high value” threshold of $50 000 per quality-adjusted life-year.
Dr Chambers concluded that the ORBIT II study showed that coronary OAS is a safe and effective treatment option in complex patients with calcified coronary lesions that is also cost-effective and potentially cost saving.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.