

Summary
The early identification of diabetes and cardiovascular disease (CVD) is essential to establish prevention strategies, which should be based on total risk for CVD. In patients with diabetes and hypertension, the current evidence supports a treatment goal of 140.90 mmHg. Coronary artery bypass grafting surgery is the optimal revascularization strategy in patients with diabetes, based on data from the FREEDOM trial.
- diabetes mellitus
- cardiovascular disease
- FREEDOM
- coronary artery bypass grafting
- coronary artery disease
- percutaneous coronary intervention
- myocardial infarction
- hypertension
- ACCORD
- cardiology & cardiovascular medicine clinical trials
- cardiometabolic disorder
In a series of presentations, 3 speakers discussed various aspects of the management of patients with diabetes mellitus (DM) and cardiovascular disease (CVD). Dan Gaita, MD, University of Medicine and Pharmacy, Timisoara, Romania, discussed the importance of identifying individuals at high risk of DM in order to reduce the risk of CVD. Habib Gamra, MD, Fattouma Bourguiba University Hospital, Monastir, Tunisia, shared data from the Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease trial [FREEDOM; Farkouh ME et al. N Engl J Med. 2012], demonstrating that coronary artery bypass grafting (CABG) surgery is the preferred method of revascularization for selected patients with DM and multivessel coronary artery disease (CAD). Finally, Tony Heagerty, MBBS, MD, University of Manchester, Manchester, England, United Kingdom, showed that there is currently no evidence for intensive glucose lowering blood pressure (BP) in these patients.
DM AND CVD
The burden of DM is increasing worldwide. As of 2011, its global prevalence was approximately 360 million and is expected to rise to 552 million by 2030 [Rydén L et al. Eur Heart J. 2013]. According to Prof Gaita, although microvascular events such as retinopathy, nephropathy, and neuropathy markedly increase the morbidity of patients with DM, it is the macrovascular complications that account for the increased mortality in this patient population.
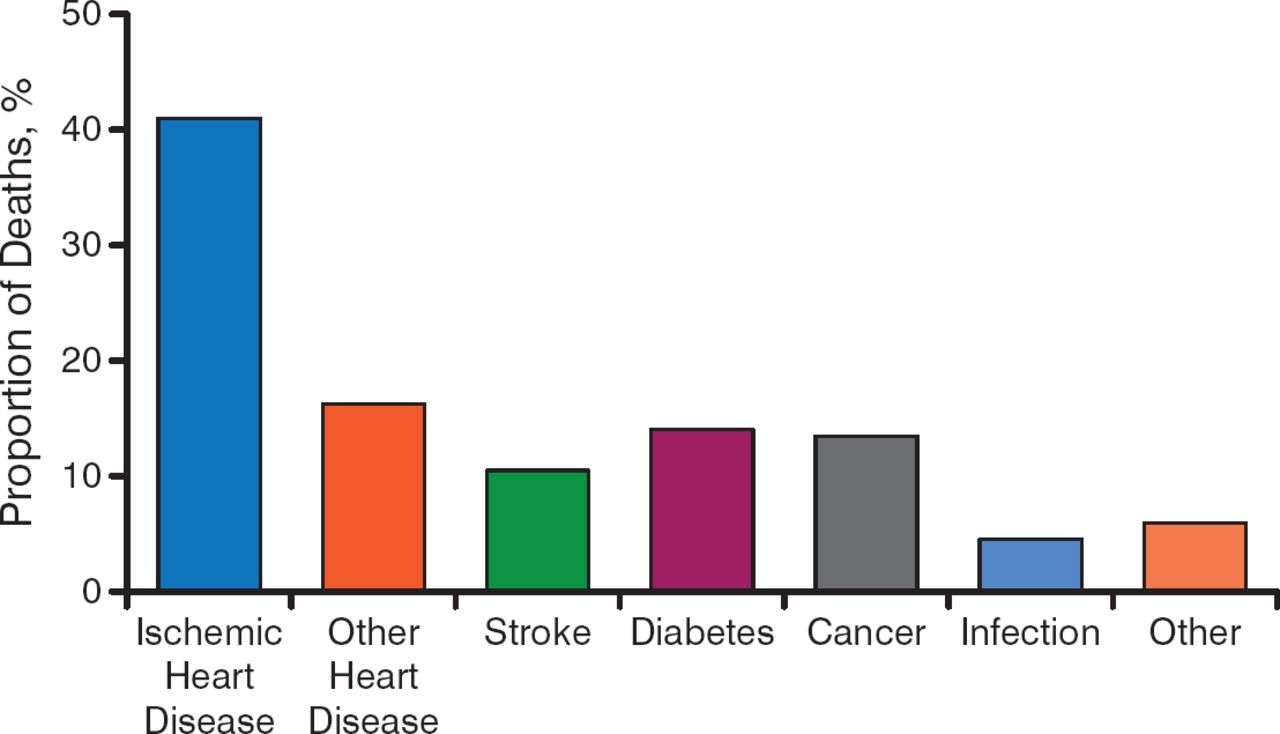
DM is a major independent risk factor for CVD, which is the leading cause of death worldwide and is the primary cause of death in patients with DM [Rydén L et al. Eur Heart J. 2013]. CVD is associated with more than one-half of the mortality (Figure 1) and a considerable amount of morbidity in patients with DM.

Cardiovascular Disease Is a Significant Cause of Mortality in Patients With Diabetes Mellitus
Adapted from Geiss LS et al. (2013). Mortality in non-insulin-dependent diabetes. In MI Harris (ed.) Diabetes in America, 2nd Edition. 233–258. Retrieved from http://diabetes.niddk.nih.gov/dm/pubs/america/pdf/chapter11.pdf. With permission from the National Diabetes Information Clearinghouse.
The economic burden of DM is also high. Hospitalization costs are driven by CVD and account for approximately 60% of medical costs in patients with DM.
During the progression to DM, the risk for macrovascular complications begins even earlier than that for microvascular complications, often up to a decade before the diagnosis of DM [Rydén L et al. Eur Heart J. 2013].
Many patients with diabetes remain undiagnosed, so screening for hyperglycemia is important in identifying high-risk individuals. Although various screening tools have been developed to screen for DM, the Finnish Diabetes Risk Score is the one most commonly used in Europe. Based on prospective data collected over 10 years, this tool predicts the 10-year risk of type 2 diabetes mellitus (T2DM) in adults with 85% accuracy.
Prof Gaita explained that it is critical to identify individuals at high risk for DM and CVD as soon as possible because appropriate lifestyle interventions can prevent the evolution from prediabetes to DM in > 70% of cases. However, he indicated that prevention of CVD should be based on total CVD risk, not just single risk factors, and he emphasized the importance of an interdisciplinary approach to patient management between diabetologists and cardiologists.
REVASCULARIZATION STRATEGIES IN PATIENTS WITH DM AND CVD
Revascularization for patients with multivessel CAD is performed commonly worldwide, and, approximately 25% of these interventions are performed in patients with DM [Farkouh ME et al. N Engl J Med. 2012]. Although CABG and percutaneous coronary intervention (PCI) are the 2 primary modalities used, the most appropriate treatment strategy has been debated.
New data from the FREEDOM trial, the largest randomized trial of PCI versus CABG in patients with DM [Farkouh ME et al. N Engl J Med. 2012], have helped to inform clinicians. This trial was conducted to determine whether CABG or PCI with drug-eluting stents is the superior approach to revascularization in patients with DM and multivessel CAD.
The trial enrolled 1900 patients (mean age 63 years) who were randomized to CABG (n = 947) or PCI (n = 953). The primary outcome was a composite of death from any cause, nonfatal myocardial infarction (MI), and nonfatal stroke. After 5 years, CABG was superior to PCI and reduced the rate of death (18.7% vs 26.6%; P = .005) and MI (6.0% vs 13.9%; P < .001), but with an increased rate of stroke (5.2% vs 2.4%; P = .03).
Although these results suggest that CABG surgery is the preferred method of revascularization for patients with DM and CAD, Prof Gamra discussed the need to use sound clinical judgment combined with collaboration and cooperation with other members of the cardiac care team to provide the best patient care. He emphasized that patient contribution in the decision making is also a key factor, stating that many of his patients still prefer PCI. Beyond the need for revascularization in patients with DM and CVD, Prof Gamra also stressed the importance of addressing other aspects of the management of these individuals, including the treatment of the DM itself and associated risk factors.
MANAGEMENT OF HYPERTENSION IN PATIENTS WITH DM
Treatment of hypertension is one important component in delaying the progression of macrovascular disease in patients with DM. According to Prof Heagerty, the guidelines have recommended a more aggressive systolic BP target of < 130 mm Hg in patients with DM compared with a target of < 140 mm Hg in those not at high risk. These recommendations were mainly based on expert consensus, with a lack of supporting evidence from randomized clinical trials. The recent Action to Control Cardiovascular Risk in Diabetes study [ACCORD; ACCORD Study Group. N Engl J Med. 2010] provided evidence for the appropriate level of BP control in T2DM.
This prospective study examined whether intensifying treatment of BP could affect residual vascular risk in individuals with T2DM (n = 4733) at high risk for cardiovascular events. Participants were randomized to intensive therapy (targeting a systolic BP < 120 mm Hg) or standard therapy (targeting a systolic BP < 140 mm Hg). The primary composite outcome was cardiovascular death, nonfatal MI, or nonfatal stroke.
After 1 year, the mean systolic BP was 119.3 mm Hg in the intensive therapy group compared with 133.5 mm Hg in the standard therapy group, and the annual rates of stroke were 0.32% versus 0.53%, respectively (HR, 0.59; 95% CI, 0.39 to 0.89; P = .01). However, there was no significant difference in the annual rates of the primary outcome (P = .20) or death from any cause (P = .55). Patients in the intensive therapy group received a mean 3.2 classes of drugs, compared with 1.9 for those in the standard therapy group, and the rate of serious adverse events associated with antihypertensive therapy was significantly higher in the intensive therapy group (3.3% vs 1.3%; P < .001).
According to Prof Heagerty, current global consensus is that unless the evidence base improves, there is no basis for intensively treating patients with DM and hypertension, and the target BP should be 140/90 mm Hg. In order to prevent diabetic nephropathy in this high-risk patient population, he recommends the use of renin-angiotensin system blockade. He concluded that angiotensin II receptor antagonists and angiotensin-converting enzyme inhibitors should be first-line drugs in these patients or in patients who require ≥ 2 drugs for BP control.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.