

Summary
This article discusses typical imaging characteristics of the uterus, endometrium, and myometrium based on patient age, reproductive cycle stage, and associated benign pathology. Other topics include the imaging of pelvic floor disorders, and imaging recommendations for the adnexa.
- magnetic resonance imaging
- diagnostic & surgical procedures
- ultrasonography
- urogenital diseases
- tomography
Reena C. Jha, MD, Georgetown University Medical Center, Washington, District of Columbia, USA, discussed typical imaging characteristics of the uterus, endometrium, and myometrium based on patient age, reproductive cycle stage, and associated benign pathology.
Postpartum physiologic changes a few days after vaginal delivery show uterine enlargement and heterogeneous engorgement of the myometrium. Cesarean delivery delays involution. Intracavitary gas has been seen in asymptomatic women as late as 3 weeks after vaginal delivery and has been noted after both vaginal and cesarean deliveries [Kamaya A et al. Ultrasound Q. 2009].
In premenopausal women, endometrial thickness and appearance vary with the phases of the menstrual cycle [Langer JE et al. Radiographics. 2012]. There are physiologic changes in the uterus seen using magnetic resonance imaging (MRI), depending on the phase of the cycle. The zonal anatomy of the uterine muscle is often less distinct on MRI during premenarche, pregnancy and up to about 6 weeks postpartum, and postmenopause. The appearance and thickness of the endometrium should be considered abnormal if they do not align with expectations for each phase of the menstrual cycle. Dr Jha noted that in a postmenopausal patient, the upper normal range of the endometrium is < 4 to 5 mm, regardless of whether she is using hormone therapy.
If the patient is bleeding and the endometrium measures ≥ 5 mm, the causes could be atrophy, polyps, or fibroids. Dr Jha then explained endometrial pathology, including polyps, tamoxifen, hyperplasia, and cancer. She noted that it is important to distinguish between how polyps and submucosal fibroids appear on the ultrasound (US; Table 1).
Differences Between Polyps and Submucosal Fibroids Using Ultrasound
Finally, Dr Jha noted that the normal thickness measurement of the junctional zone, based on histologic studies, is < 8 mm. If the junctional zone is > 12 mm, a diagnosis of adenomyosis is likely. The results of 1 meta-analysis showed that a correct diagnosis of adenomyosis was obtained more often with MRI than with US [Champaneria R et al. Acta Obstet Gynecol Scand. 2010]. Adenomyosis can mimic fibroids, uterine contractions, and invasive endometriosis.
AN UNDERREPORTED QUALITY-OF-LIFE ISSUE: PELVIC FLOOR DISORDER
Mark Lockhart, MD, MPH, University of Alabama, Birmingham, Alabama, USA, discussed pelvic floor disorders, which are an underreported health problem with a major impact on quality of life.
By the year 2050, 43.8 million American women will have at least 1 symptomatic pelvic floor disorder, 28.4 million will have urinary incontinence, 16.8 million will suffer from fecal incontinence, and 4.9 million will live with pelvic organ prolapse [Wu JM et al. Obstet Gynecol. 2009]. Risk-based factors for pelvic floor disorder include multiple vaginal deliveries, trauma, and obesity. Older women are particularly hard hit: 37% of those aged 60 to 79 years and 50% of those aged ≥ 80 years had at least 1 pelvic floor disorder based on 2005 to 2006 National Health and Nutrition Examination Survey data [Nygaard I et al. JAMA. 2008].
Thorough preoperative assessment of pelvic floor failure is necessary to reduce the rate of relapse, which is reported to be as high as 30% [Bitti GT et al. Radiographics. 2014].
Imaging options include defecography, cystography, US, and dynamic MRI. Dynamic MRI is a powerful tool that enables radiologists to comprehensively evaluate pelvic anatomic and functional abnormalities, thereby helping surgeons to provide appropriate treatment and avoid repeat surgeries. Magnetic resonance defecography changed surgical plans in 67% of patients who underwent fecal incontinence surgeries [Hetzer FH et al. Radiology. 2006].
Indications for MRI include anal incontinence (sphincter evaluation); anal symptomology, pain, or mass; pelvic organ prolapse (difficult physical examination or suspicion or multicompartment damage); and failed prior surgery. According to Dr Lockhart, the MRI technique calls for a collapsed bladder and the insertion of US gel into the rectum. The patient is supine for 20 to 30 minutes, with a center-phased array coil on the low pelvis.
Technical considerations include the use of an internal vs external anal coil, the volume of rectal contrast, repeated strain vs defecography, static images vs cine clips, filling of the vagina and small bowel, empty vs filled bladder, pubococcygeal vs midpubic line, and 1.5 vs 3.0 T. Defecation phase images can be very useful in identifying additional instances of abnormal bladder, vaginal, and rectal descent [Flusberg M et al. AJR Am J Roentgenol. 2011].
Dr Lockhart concluded that improvement is needed in the standardization of MRI examinations and interpretation criteria. Future trends will focus on 3D imaging, automation and standardization, postsupport imaging, strain vs evacuation criteria, and reduction of interpretation variability.
IMAGING THE ADNEXA
Maitray D. Patel, MD, Mayo Clinic Arizona, Scottsdale/Phoenix, Arizona, USA, spoke on imaging recommendations for the adnexa. He outlined an algorithm for thinking about an adnexal mass, reviewed the 2009 Society of Radiologists in Ultrasound (SRU) consensus recommendations for managing simple cysts identified by US [Levine D et al. Ultrasound Q. 2010], and also discussed the American College of Radiology (ACR) recommendations for managing incidental ovarian findings on computed tomography (CT) images [Patel MD et al. J Am Coll Radiol. 2013].
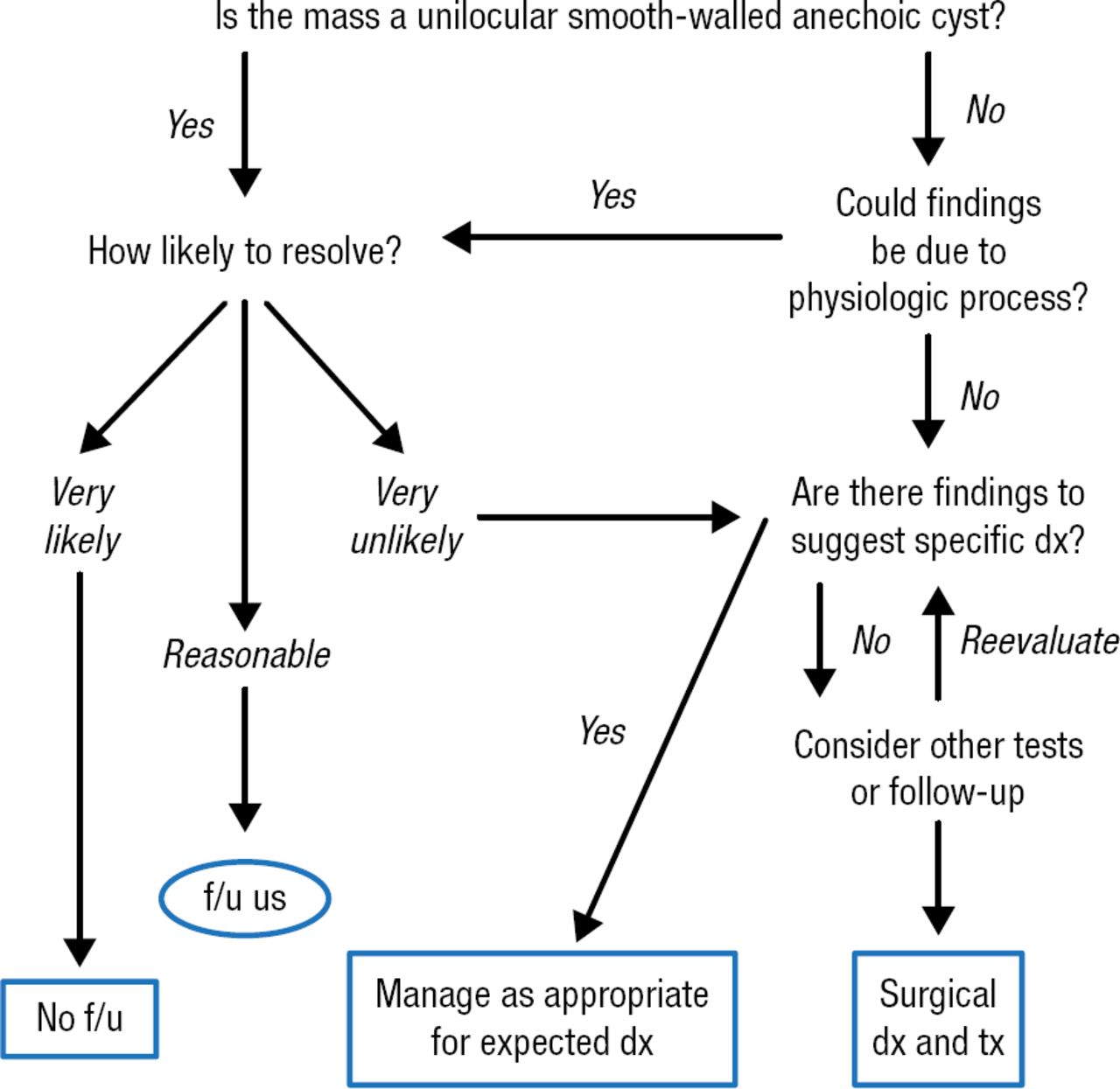
Dr Patel first discussed an algorithm that can help analyze and understand adnexa pathology. He used this as the basis of his presentation (Figure 1).

Suggested Approach to an Adnexal Mass Identified by US
dx, diagnosis; f/u, follow-up; tx, treatment; us, ultrasound.
Adapted with permission of Elsevier Inc, from Patel MD. Practical Approach to the Adnexal Mass.
Ultrasound Clin. 2006;1:335–356. Permission conveyed through Copyright Clearance Center, Inc.
According to Dr Patel, imaging impressions regarding an adnexal mass are paramount in determining case management particularly because the majority of adnexal masses in premenopausal women will be nonneoplastic ovarian cysts that will spontaneously resolve, usually within 2 menstrual cycles. These nonneoplastic adnexal cysts can also be found in postmenopausal women. In postmenopausal women, up to 50% usually resolve within 1 to 2 years, with resolution more common in women who have been postmenopausal < 10 years [Castillo G et al. Gynecol Oncol. 2004]. Therefore, imagers must be well versed in recognizing adnexal masses that do not require intervention or further imaging.
The risk of malignancy in simple adnexal cysts (unilocular adnexal cysts without internal echoes) measuring < 10 cm in diameter is extremely low [Modesitt SC et al. Obstet Gynecol. 2003]. In a study of about 3000 unilocular cysts measuring < 10 cm in > 15 000 in postmenopausal women, < 0.1% had a risk of malignancy. In that study, rare malignancies were all borderline malignancies and always > 5 cm and had identified septations or tiny wall nodules recognized at follow-up.
The SRU consensus recommendation for managing incidental simple cyst identified on US are based on the following criteria: a simple cyst does not require further imaging evaluation or follow-up if the patient is asymptomatic and the cyst is either ≤ 5 cm in premenopausal patients or < 1 to 3 cm in postmenopausal women [Levine D et al. Ultrasound Q. 2010]. Dr Patel noted that the SRU criteria allow that imagers can choose any cutoff value between 1 and 3 cm as valid for not following a simple cyst in a postmenopausal woman. Asymptomatic simple cysts between 5 and 7 cm in diameter can be safely followed with yearly US. When simple cysts are > 7 cm in diameter, the SRU criteria suggest that magnetic resonance evaluation and/or surgical consultation can be pursued.
A CT of the pelvis is commonly performed prior to US when a patient is presenting with acute pain in the emergency room, suspected bowel pathology, and suspected renal calculi. The ACR recommendations should be used when managing incidental findings on abdominal and pelvic CT and MRI.
Reimaging with US refers to when the US is performed immediately or within a few days of CT to further characterize a CT finding or suspected clinical entity. Follow-up imaging with US refers to when US is performed after some interval from the CT, to assess the effect of time on a detected finding [Patel MD, Dubinsky TJ. Ultrasound Q. 2007]. Dr Patel emphasized that neither reimaging nor follow-up imaging should be necessary when the CT scan shows gynecologic structures to be normal; when an incidental finding is identified in which the differential diagnosis is a nonneoplastic cyst vs a benign neoplasm, reimaging is not helpful, as one needs to understand the evolution of the finding over time (requiring follow-up imaging rather than reimaging).
Dr Patel summarized by emphasizing the importance of developing a conceptual framework for managing decisions on how to assess the type of cysts in patients.
- © 2015 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.