

Summary
Exercise causes a complex interplay to occur between multiple major organs including the brain, heart, and skeletal muscles. The proficiency with which these organs work together during exercise is measured by cardiorespiratory fitness, a measure of maximal oxygen intake (VO2 peak). This article provides an overview of exercise physiology in regards to stroke rehabilitation, the consequences of stroke on metabolic health and skeletal muscle, the role of physical activity within the first week after stroke, as well as describes how poststroke exercise training is of benefit to stroke survivors.
- Nursing
- Cardiometabolic Disorder
- Cerebrovascular Disease
- Neurology
- Nursing
- Cardiometabolic Disorder
- Cerebrovascular Disease
Exercise causes a complex interplay to occur between multiple major organs including the brain, heart, and skeletal muscles. The proficiency with which these organs work together during exercise is measured by cardiorespiratory fitness, a measure of maximal oxygen intake (VO2 peak). Importantly, patients who have experienced stroke demonstrate a VO2 peak that is ∼60% lower than age- and sex-matched controls [Mackay-Lyons MJ et al. Arch Phys Med Rehabil 2002]. In addition, patients who have experienced stroke have reduced activity levels due to decreased physical function, mobility, and activities of daily living because they have a limited oxygen reserve. Sandra A. Billinger, PT, PhD, University of Kansas Medical Center, Kansas City, Kansas, USA, provided an overview of exercise physiology in regards to stroke rehabilitation.
An important question that healthcare providers should ask is when to initiate an exercise program in their stroke patients. The Aerobic Exercise Recommendations to Optimize Best Practices in Care After Stroke [AEROBICS; Mackay-Lyons M et al. http://strokebestpractices.ca/wp-content/uploads/2013/07/AEROBICS-FINAL-July-2013.pdf] suggests that patients should be screened as soon as their neurologic and cardiopulmonary statuses are stable. Dr. Billinger pointed out that at this point, the recommendation to the patient may be as simple as getting out of bed to use the restroom or to sit in a chair.
In the Cardiovascular Regulation, Exercise in Subacute Stroke study [CRESS; Billinger SA et al. J Neurol Phys Ther 2012], 10 patients within 4 months post stroke were enrolled for 8 weeks of aerobic exercise 3 times per week. Exercise was performed using a recumbent stepper and the heart rate reserve was measured at 4 and 8 weeks. Although the initial goal was to reach 20 mL*kg-1*minute-1, the VO2 peak significantly increased from 15.8 at baseline to 17.5 mL*kg-1*minute-1 following the intervention (p=0.04; Table 1). A significant increase in the work performed by the patients, as measured by watts, also increased from 66.7 to 83.3 (p=0.004).
Peak Exercise Hemodynamic Measures From the CRESS Study
Alice S. Ryan, PhD, University of Maryland School of Medicine, Baltimore, Maryland, USA, presented information about the consequences of stroke on metabolic health and skeletal muscle. Patients who survive stroke have a decreased fitness reserve compared with healthy, sedentary controls [Ivey FM et al. Neuro Rx 2006]. Metabolic health plays an important role in stroke recurrence, as stroke survivors with impaired glucose tolerance (IGT) and type 2 diabetes mellitus (T2DM) have a 2- to 3-fold greater risk for stroke recurrence [Vermeer SE et al. Stroke 2006]. Importantly, ∼81% of patients who have experienced stroke have IGT or T2DM [Ivey FM et al. Cerebrovasc Dis 2006]. Glucose intolerance is associated with decreased capillary density, and the capillary density within skeletal muscle is decreased in both the nonparetic and paretic skeletal muscle in stroke survivors [Prior SJ et al. Microcirculation 2009].
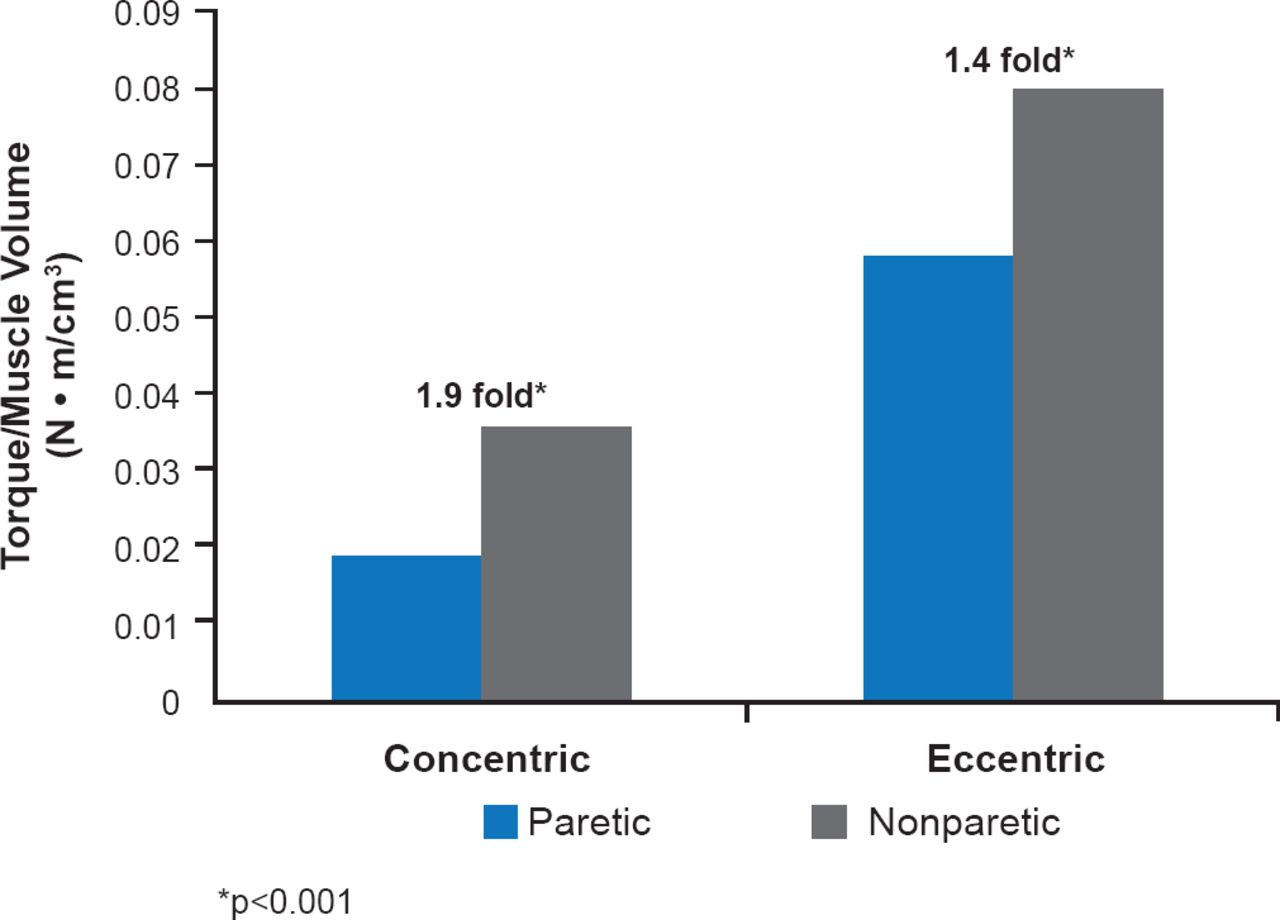
Muscle atrophy is apparent in patients who have survived stroke, and paretic thigh atrophy is associated with low fitness [Ryan AS et al. J Stroke Cerebrovasc Dis 2000]. In one study, paretic muscle area decreased by 20% (p<0.001), whereas paretic intramuscular fat increased by 25% (p<0.0001) following stroke [Ryan AS et al. Arch Phys Med Rehabil 2002]. In stroke survivors, the paretic leg has reduced muscle quality, as measured by torque divided by muscle area; the paretic leg has about a 2-fold lower muscle quality than the nonparetic leg (Figure 1) [Ryan AS et al. Neurorehabil Neural Repair 2011].

Muscle Quality in Paretic Versus Nonparetic Legs
Source: Ryan AS et al. Atrophy and intramuscular fat in specific muscles of the thigh: associated weakness and hyperinsulinemia in stroke survivors. Neurorehabil Neural Repair 2011;25(9):865–872.
Sarcopenia is the reduction of skeletal muscle mass and function as a result of aging. In a study of over 200 stroke survivors between the ages of 45 and 84 years with a wide range of body weight, 13% and 21% of patients aged 61 to 70 and 71 to 80 years, respectively, had sarcopenia compared with 13% and 24% of nonstroke controls. However, when a sample of the stroke patients were matched to nonstroke controls based on age, body mass index, gender, and ethnicity, patients who had experienced stroke demonstrated a reduced skeletal muscle index compared with the controls (p<0.0001) with a sarcopenia prevalence of 12.8% and 5.1%, respectively.
As a result of muscle abnormalities and muscle adaptions that occur as a result of stroke, it is a logical approach to target skeletal muscle for rehabilitation after a stroke event. Aerobic training, such as treadmill walking, improves both VO2 peak and economy of gait in stroke survivors compared with controls [Macko RF et al. Stroke 2005]. Resting blood flow also improves in the paretic and nonparetic legs following aerobic training in stroke survivors [Ivey FM et al. Stroke 2010]. In addition, aerobic training decreases both plasma glucose and insulin concentrations compared with controls, with over half of the patients reversing their IGT or T2DM status [Ivey FM et al. Stroke 2007]. Resistive training, in which patients perform high-volume, high-intensity and progressive exercise, also was beneficial to stroke patients. Resistive training improved leg strength, muscle hypertrophy, and muscle attenuation [Ryan AS et al. Stroke 2011] as well as insulin sensitivity [Ivey FM, Ryan AS. J Stroke Cerebrovasc Dis 2014].
Toby Cumming, BBSc, PhD, Florey Institute of Neuroscience and Mental Health, Melbourne, Australia, discussed the role of physical activity within the first week after stroke. Animal studies demonstrate that earlier exercise reduces infarct volume and improves neurobehavioral score after stroke [Egan KJ et al. Neurorehab Neural Repair 2014]. In a study of 100 humans within 24 hours of stroke, patients were mobilized out of bed and monitored in a sitting position for the following hour [Indredavik B et al. ESC 2007 (poster)]. The procedure was shown to be safe, with potential beneficial effects attributable to heightened level of consciousness, increased oxygen saturation and transient elevation of blood pressure.
In an ongoing study, Prof. Cumming and colleagues are evaluating energy expenditure by fitting acute stroke patients with a portable metabolic calorimeter and 2 SenseWear armbands. Patients are asked to do 2 bouts of exercise for 6 minutes each: either walking or repeated sit-to-stands. Preliminary results indicate that achieving steady state exercise is feasible in the days after stroke and that energy expenditure levels are in the expected range (8 to 12 mL VO2/kg/minute). However, Prof. Cumming pointed out that even if acute stroke patients have the same energy expenditure as non-stroke controls, they may experience greater fatigue. Data from this study will have important implications for the introduction of physical rehabilitation early after stroke.
Gillian E. Mead, MB, BChir, MA, MD, University of Edinburgh, Edinburgh, United Kingdom, described how poststroke exercise training is of benefit to stroke survivors. A recent Cochrane review of fitness training post stroke indicated that physical fitness, walking, and functioning were improved and disability was reduced [Saunders DH et al. Cochrane Database Syst Rev 2013]. It is highly likely that exercise will also reduce the risk of recurrent vascular events. However, there are multiple barriers to exercise after stroke. A systematic review of 174 patients found that lack of motivation; environmental factors such as transport, cost, and access; as well as health concerns and disabilities due to stroke prevented patients from performing exercise [Nicholson S et al. Int J Stroke 2012]. However, social support, the improved ability to carry out normal every day tasks, and professional facilitators guiding exercise served as motivators. A recent qualitative interview study with 13 stroke survivors highlighted beliefs about their capability to exercise, and environmental context and resources as the greatest barriers to exercise. If health and exercise professionals can remove barriers to exercise, uptake should be increased.
Prof. Mead introduced a stroke specialist instructor course that focuses on training exercise professionals to guide and facilitate exercise in stroke survivors. The program has received endorsements from multiple organizations in the United Kingdom and the course for exercise professionals is now available from Later Life Training (www.laterlifetraining.co.uk). Patients that survive stroke undergo screening for exercise after being discharged from the hospital and then complete a pre-exercise assessment. Once a patient is cleared for exercise, the patient participates in specialized exercise sessions at their local gym. Prof. Mead described an innovative new program to bring exercise professionals onto an acute stroke unit; to join the multidisciplinary stroke team, to promote the benefits of long-term exercise and to bridge the gap between hospital stroke services and community exercise after stroke services. This program was set up in collaboration with Edinburgh Leisure (Scotland).
Stroke survivors often experience significant morbidity that results in reduced functioning and mobility. Introducing movement and exercise early following stroke improves a range of clinical outcomes. It is now time to implement exercise training into clinical practice.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.