

Summary
The RIVAL study demonstrated that the transradial approach for percutaneous coronary intervention was as safe and effective as the transfemoral but was associated with a lower rate of vascular complications. Importantly, the effectiveness of the transradial approach was related to procedure volume and previous experience. The Czech PCI Registry found that the incidence of 30-day death was lower with the transradial approach in patients with STEMI and NSTEMI.
- transradial approach
- transfemoral approach
- percutaneous coronary intervention
- RIVAL
- NCT01014273
- unstable angina
- myocardial infarction
- acute coronary syndromes
- STEMI
- coronary artery bypass graft
- cardiology & cardiovascular medicine clinical trials
Petr Kala, MD, PhD, Masaryk University and University Hospital Brno, Brno, Czech Republic, shared data from A Trial of Trans-radial Versus Trans-femoral Percutaneous Coronary Intervention (PCI) Access Site Approach in Patients With Unstable Angina or Myocardial Infarction Managed With an Invasive Strategy [RIVAL; NCT01014273], demonstrating that the transradial approach (TRA) and the transfemoral approach (TFA) are both safe and effective for PCI. TRA reduced the rate of vascular complications; however, the effectiveness of TRA is linked to the volume and prior expertise.
According to Prof Kala, TFA has traditionally been the primary route of arterial access for cardiac catheterization. TRA represents an alternative access site that has some advantages over femoral access. Because of decreased vascular and bleeding complications, both the American College of Cardiology Foundation/American Heart Association guidelines on PCI [Levine GN et al. J Am Coll Cardiol. 2011] and the European Society of Cardiology guidelines on management of acute coronary syndromes (ACSs) in patients Non-STE ACS support the use of TRA by experienced operators when feasible [Hamm CW et al. Eur Heart J. 2011].
The RIVAL trial was the largest study to compare the efficacy and safety of the TRA with TFA in patients being treated with an invasive strategy for an ACS [Jolly SS et al. Lancet. 2011]. In this multicenter, randomized, parallel-group study, between June 6, 2006 and November 3, 2010, patients (n = 7021) with an ACS were randomized to either TRA (n = 3507) or TFA (n = 3514). In order to be included, patients had to have intact dual circulation of the hand. The procedures were performed by interventional cardiologists experienced in both techniques. The primary end point of the trial was the composite of death, myocardial infarction (MI), stroke, or non–coronary artery bypass grafting (CABG)-related major bleeding at 30 days.
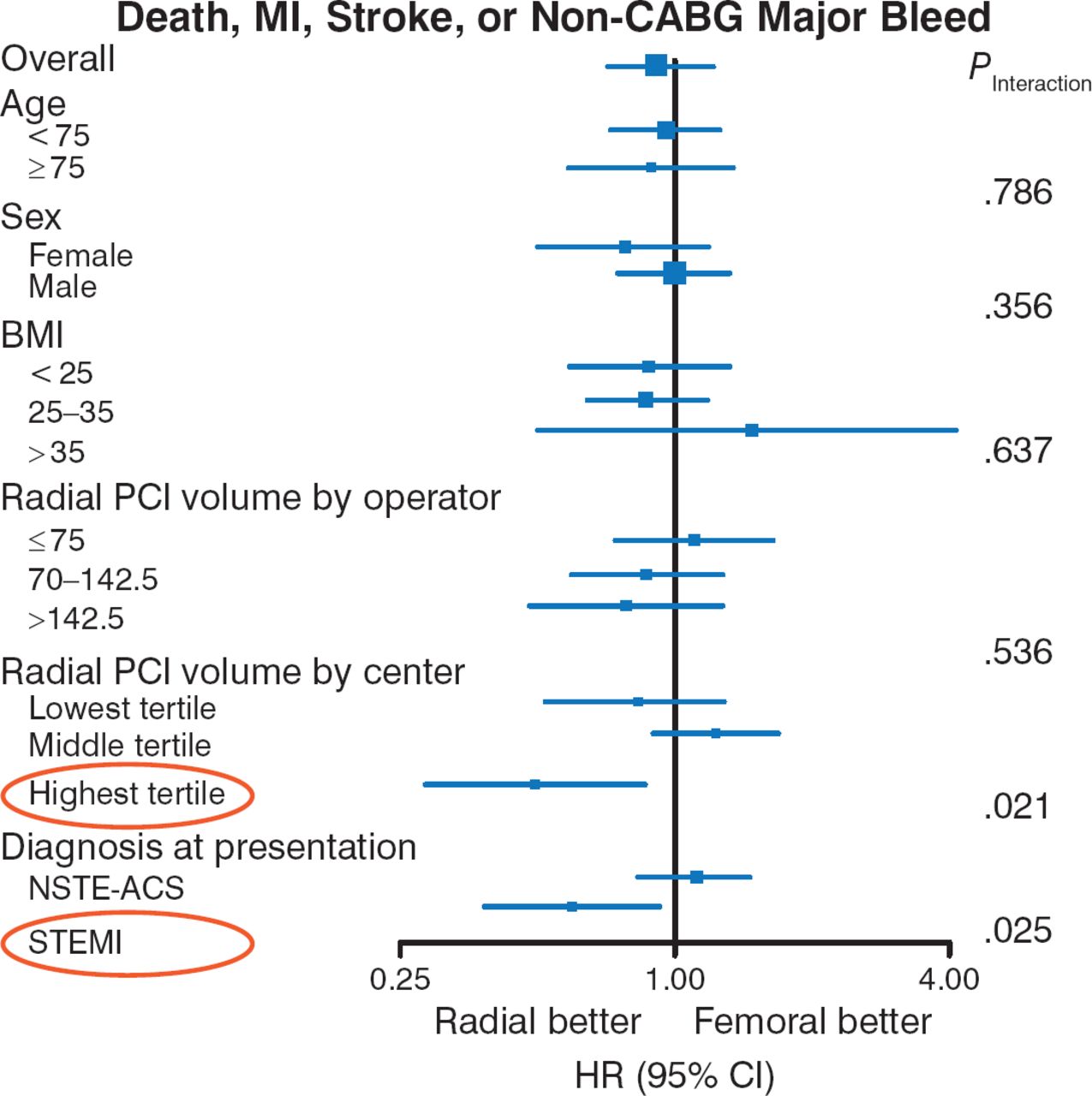
The results of the study showed that there was no statistical difference in the rate of the primary end point between TRA and TFA groups (3.7% vs 4.0%; P = .50). TRA decreased major vascular complications (1.4% vs 3.7%; P < .0001). Access site crossover was higher in the TRA group (7.6% vs 2.0%; P < .0001). In subgroup analyses, rates of primary outcome also appeared to be lower in the TRA group in high-volume radial centers (P = .021) and STEMI (P = .025; Figure 1).

Subgroups Analyses for the Primary Outcome
BMI, body mass index; CABG, coronary artery bypass graft; MI, myocardial infarction; NSTE/ACS, non–ST-segment elevation acute coronary syndrome; PCI, percutaneous coronary intervention.
Adapted from The Lancet, 377. Jolly SS et al. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomised, parallel group, multicentre trial. 1409–1420. Copyright 2011, with permission from Elsevier.
Prof Kala discussed the current state of TRA for PCI in the Czech Republic. He presented unpublished data from the Czech PCI Registry in the National Register of Cardiovascular Interventions containing information from all PCI procedures (> 100 000) that were performed in the country since 2005. The use of TRA has been increasing annually and was used in 70% of PCI cases in 2013 [Kala P. ESC Proceedings. 2014].
The registry was used to compare data and outcomes associated with use of the TRA and TFA. As compared to patients treated with TFA, patients in whom TRA was used had a lower incidence of prior MI (27% vs 30%; P < .001), PCI (11% vs 13%; < 0.001), heart failure (7.3% vs 6.6%; P = .002), and CABG. Patients treated with TRA had lower rates of death at 30 days (2% vs 3%; P < .001). Interestingly, Prof Kala noted that this difference in all-cause mortality was significant for in patients with STEMI (1% vs 3%; P < .001) and non-ST segment elevation. Prof Kala concluded by noting that these data suggest that the TRA is feasible in patients undergoing PCI, including those with ACS.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.