

Summary
Atrial fibrillation can become self-sustaining due to structural remodeling that results in changes in ion currents over time. Treatment of atrial fibrillation with ablation does not appear to be improved by additional substrate ablation (CFE or Lines) when performed in addition to PVI. There is also mounting evidence for the role of rotors in AF. Many patients experience termination of atrial fibrillation following ablation of rotor sites, suggesting that therapies that target rotors may be one approach to reduce the burden of AF.
- atrial fibrillation
- CFE
- complex fractionated electrogram ablation
- eplerenone
- FIRM
- focal impulse and rotor modulation
- pulmonary vein isolation
- PVI
- rotor
- STAR AF II
- cardiology & cardiovascular medicine clinical trials
- interventional techniques & devices
Atrial fibrillation (AF) is the most common atrial arrhythmia and a strong independent risk factor for stroke, heart failure, and death. Catheter ablation is an established treatment to achieve and maintain sinus rhythm in patients with recurrent AF. However, persistent AF is resistant to ablation and medical therapy, creating an unmet medical need in treatment of this disorder.
Self-sustaining Persistent Atrial Fibrillation
Stanley Nattel, MD, Montreal Heart Institute, Montreal, Quebec, Canada, presented an overview of longstanding persistent AF.
AF becomes self-sustaining and perpetuates itself in the short term by causing ion current changes and action potential duration shortening that promotes reentrant arrhythmias. However, this factor alone is not sufficient to cause longstanding persistent AF. Structural remodeling is also essential for the development of this disorder, and tissue fibrosis is a major component of the process [Martins RP et al. Circulation. 2014]. There is a progressive increase in atrial fibrosis as AF becomes increasingly persistent. Fibrosis, particularly in epicardium, separates myocytes and creates conduction barriers [Verheule S et al. Circ Arrhythm Electrophysiol. 2010].
While the changes in the electrical component are reversible after AF termination, the structural changes reverse slowly and in some patients do not occur at all [Haissaguerre M et al. Circulation. 2014]. Such tissue remodeling can accumulate over time, leading to longstanding AF. However, other factors such as cardiovascular disease and normal aging can also cause structural changes that promote AF.
Elucidation of the mechanism of AF development led to some clinical attempts to target upstream factors in order to prevent the progression of fibrosis in patients with longstanding persistent AF.
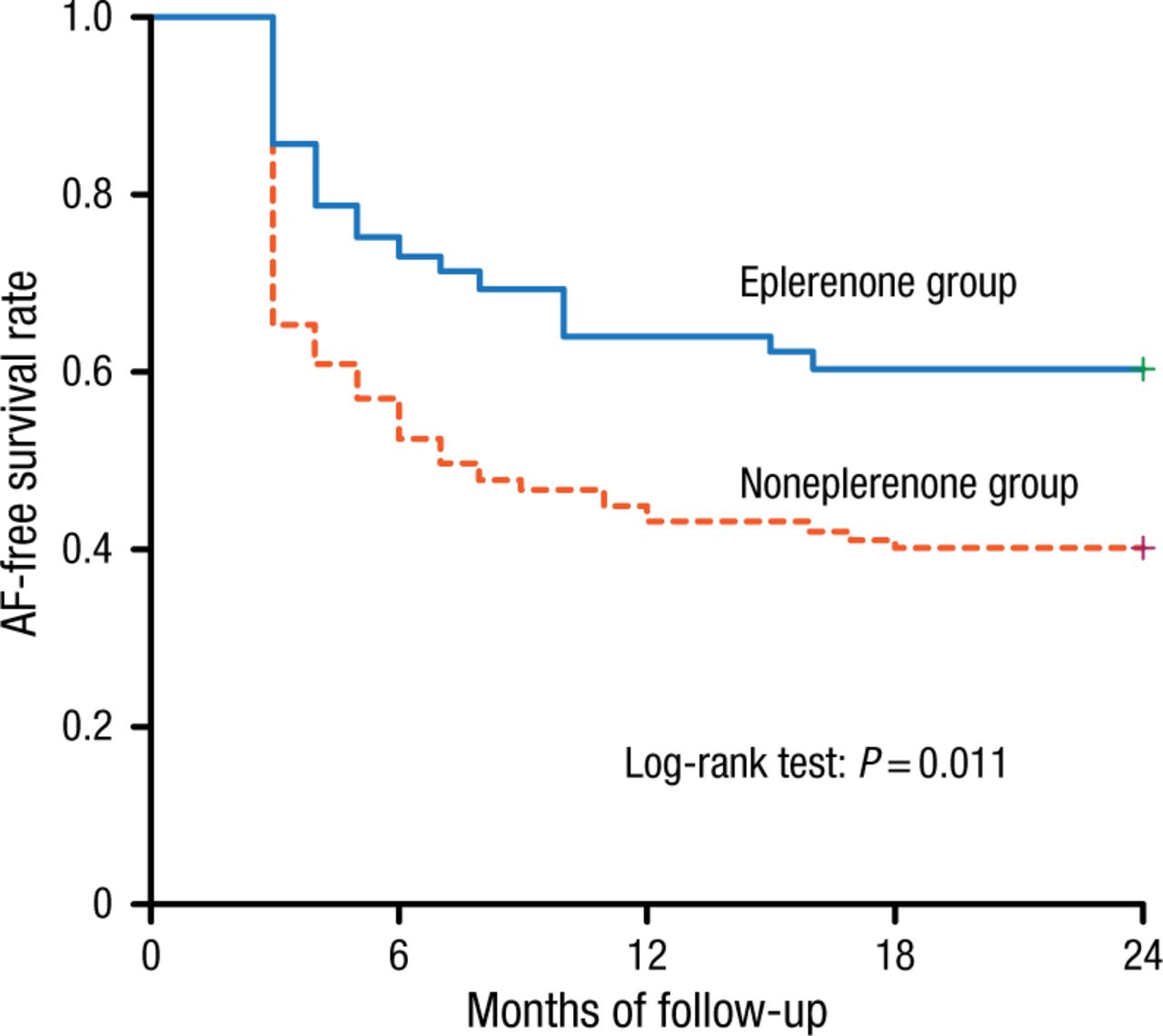
A study by Ito and colleagues [Am J Cardiol. 2013] evaluated the effects of eplerenone, a selective aldosterone blocker, on clinical outcomes after radiofrequency catheter ablation in patients with longstanding persistent AF (n = 161). After 24 months of follow-up, the rate of freedom from AF recurrence was significantly higher in the eplerenone group than in the control group (60% vs 40%, respectively; P = .011; Figure 1).

Atrial Fibrillation–Free Survival by Treatment
Kaplan-Meier curves showing the rate of freedom from AF recurrence in the eplerenone and noneplerenone groups during 24-month follow-up.
Reprinted from Am J Cardiol, Vol. 111, Ito Y et al, Effect of Eplerenone on Maintenance of Sinus Rhythm After Catheter Ablation in Patients With Long-Standing Persistent Atrial Fibrillation, Pages No. 1012-1018, Copyright (2013), with permission from Elsevier.
Other studies have attempted to address AF risk factors in hopes that such interventions would reduce the prevalence of AF and alleviate AF burden. In a partially blinded, randomized controlled study by Abed and colleagues [JAMA. 2013], 150 patients were randomized to either weight management (intervention) or general lifestyle advice (control). Weight reduction resulted in reduced AF symptom burden and severity and in beneficial cardiac remodeling after a 15-month follow-up. Managing obstructive sleep apnea, another risk factor for AF, was associated with a lower recurrence of AF in a prospective study that included 153 patients who underwent extensive encircling pulmonary vein isolation (PVI) for drug-refractory AF [Naruse Y et al. Heart Rhythm. 2013].
Dr Nattel concluded that strategies to improve outcomes include earlier and more effective interventions, aggressive risk factor management, and potential therapies that prevent substrate progression.
Ablation of Persistent Atrial Fibrillation
Ablation of AF is challenging and usually less successful for persistent AF than for paroxysmal AF. The European Heart Rhythm Association/Heart Rhythm Society guidelines on cardiac resynchronization therapy in heart failure suggest that more extensive ablation should be considered [Daubert JC et al. Heart Rhythm. 2012]; however, it remained unclear whether more extensive ablation improves outcomes.
Atul Verma, MD, Southlake Regional Health Center, Newmarket, Ontario, Canada, presented results of the STAR AF II trial [Verma A et al. N Engl J Med. 2015], demonstrating that there was no reduction in the rate of recurrent AF with either linear ablation (Lines) or ablation of complex fractionated electrograms (CFEs) performed at the time of PVI in patients with persistent AF.
STAR AF II was a multicenter, prospective, randomized trial with the objective to compare the efficacy of 3 different catheter ablation strategies in patients with persistent AF: PVI alone vs PVI plus CFE vs PVI plus Lines. The primary end point was freedom from documented AF lasting > 30 seconds at 18 months after 1 or 2 ablation procedures with or without antiarrhythmic medications.
A total of 589 patients were randomized 1:4:4 to PVI, PVI plus CFE, and PVI plus Lines, respectively. Successful PVI was performed in 97% of patients across all groups, CFEs were eliminated in 80%, and bidirectional block across both roof and mitral lines was achieved in 74%.
After 18 months, 59% of patients assigned to PVI alone were free from recurrent AF compared to 49% of patients assigned to PVI plus CFE and 46% of patients assigned to PVI plus Lines (P = .15). There were no significant differences between the groups in regard to the secondary end points, including freedom from AF after 2 ablation procedures and freedom from any atrial arrhythmia. AF burden was reduced significantly in all treatment groups. Complications were rare and did not differ significantly between the groups.
Dr Verma concluded that in the largest randomized trial to date evaluating the methods of AF ablation, there was no reduction in AF when additional substrate ablation (CFE or Lines) was performed in addition to PVI. Novel targets for ablation may include rotors, repetitive patterns, and non-PVI foci.
The Role of Rotors in Atrial Fibrillation
Omer Berenfeld, PhD, University of Michigan Health System, Ann Arbor, Michigan, USA, and Michel Haïssaguerre, MD, University of Bordeaux, Talence, France, discussed rotors and their role in AF mechanisms and treatment.
Rotors are a special type of reentrant circuits of action potentials possibly revolving around a normally excitable core; in contrast with the reentries in which the wavefront and wavetail do not meet, the curved front and tail of the rotor meet each other near their pivoting tip. Rotors are difficult to study, mainly because of the low voltage amplitude at their core and their tendency to meander and drift, prompting phase and frequency domain algorithms for their mapping [Rodrigo M et al. Heart Rhythm. 2014].
Various mapping methods have been developed to detect and map rotor activity in humans. A more invasive method involves the use of a basket catheter [Narayan SM et al. J Am Coll Cardiol. 2012]. The catheter provides localized atrial mapping but does not capture all tissue surface. Body surface mapping and electrocardiographic imaging are less invasive and provide panoramic biatrial mapping, but do not capture smaller signals [Rodrigo M et al. Heart Rhythm. 2014].
A mechanistic role of rotors in AF is suggested by termination and freedom from AF following the ablation of rotor sites. Treatment of AF in the CONFIRM trial [Narayan SM et al. J Am Coll Cardiol. 2012] (n = 92) resulted in AF termination or consistent slowing in 86% of patients who underwent targeted focal impulse and rotor modulation vs 20% of those treated by conventional ablation alone.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.