

Summary
Although liver biopsy is considered the gold standard method of assessment for liver fibrosis, it is being displaced by noninvasive testing, such as serum biomarkers, vibration-controlled transient elastography, magnetic resonance elastography, and acoustic radiation force impulse. However, it is important to understand how they perform, particularly in patients with stage 2 to 3 fibrosis.
- fibrosis
- cirrhosis
- liver disease
- hepatitis C virus
- HCV
- hepatitis B virus
- HBV
- biopsy
- noninvasive testing
- magnetic resonance elastography
- transient elastography
- acoustic radiation force impulse
- imaging modalities
Although liver biopsy is the traditional gold standard for evaluating liver fibrosis, other noninvasive methods have become important tools for assessment, such as biomarkers and various imaging modalities. Nezam H. Afdhal, MD, Beth Israel Deaconess Medical Center, Boston, Massachusetts, USA, discussed methods of assessing liver fibrosis.
Not only can liver biopsy identify fibrosis, but it can also provide information about the severity of hepatitis C virus (HCV), as well as the presence of other problems, such as steatosis, granulomatous processes, and autoimmune diseases. These findings cannot be identified with noninvasive testing. However, Dr Afdhal pointed out that biopsy does not provide a lot of new data in regard to diagnosis, staging, and prognosis. In addition, it is difficult and time-consuming; it carries risks; and it may not actually be needed with current therapies, at least for patients with HCV.
The Ishak scoring system translates pathologic appearance of a liver biopsy into a stage (Table 1). Although this system is ideal for clinical trials where comparisons among patients is required, Dr Afdhal stated that the problem with all scoring systems in everyday clinical practice is that they do not correlate with collagen staining, which is the true marker of fibrosis. This is one reason why noninvasive imaging is more accurate for identifying fibrosis; it measures fibrosis and does not attempt to fit the results into a scoring system.
Stage Component of the Ishak System
In addition, the reproducibility of biopsy results is low, at least in part due to an inadequate-sized biopsy and to interobserver variation in the interpretation of the results, particularly for the F1 through F3 stages.
Yet, the measurement of fibrosis is needed for cross-sectional assessment of liver disease and to monitor the change in disease over time. In addition, knowledge of fibrosis severity enables clinicians to identify and talk to patients about risk factors. For example, advanced cirrhosis increases the risk of hepatocellular carcinoma (HCC), which is an important topic to discuss with patients. Furthermore, the 2005 American Association for the Study of Liver Disease practice guideline for the management of HCC recommends that patients who are at high risk of developing HCC should undergo surveillance [Bruix J et al. Hepatology. 2005]. The association’s 2007 guideline recommends screening for esophageal and gastric varices in patients with cirrhosis [Garcia-Tsao G et al. Hepatology. 2007]. Noninvasive methods of fibrosis staging are able to provide this information.
There are multiple noninvasive methods to assess fibrosis—including serum biomarkers, vibration-controlled transient elastography, magnetic resonance elastography (MRE), acoustic radiation force impulse, diffusion-weighted magnetic resonance imaging, weighted computed tomography mean fibrosis, and combinations of the above. There are multiple scores produced from biomarkers for both HCV and hepatitis B virus, such as the FibroTest, ELF, and FibroSpect.
The AST to Platelet Ratio Index (APRI) has an area under the curve of 0.88 for livers with an Ishak score ≥ 3. About 30% of patients have an APRI score < 0.5 and 22%, a score of ≥ 1.5; furthermore, 86% and 88% of the time, respectively, these cases are correctly identified according to an Ishak score of < 3 and ≥ 3. However, about 50% of people are not correctly classified with the APRI. Dr Afdhal pointed out that the performance is similar among other serum biomarker diagnostic tests, particularly around the range of stage 2. Correct classification of the fibrosis stage can be increased by combining serum biomarker tests [Boursier J et al. Liver Int. 2009]; if the APRI is not conclusive, subsequent testing with the FibroTest/FibroSure can increase correct classification to about 70%, and the remaining 30% can undergo liver biopsy [Sebastiani G et al. Hepatology. 2009].
The serum biomarker tests also perform similarly to liver biopsies as a prognostic indicator. Dr Afdhal stated that all of the serum tests are excellent at predicting overall survival, as well as survival with or without liver events [Poynard T et al. Gastroenterol Hepatol. 2011]. Therefore, he suggested that a combination of different and unrelated tests can be used to improve the accuracy of staging, with liver biopsy reserved for patients whose staging is inconclusive or borderline. However, he pointed out that most of these tests were validated in patients with HCV and do not perform as well in patients with hepatitis B virus or other liver disease.
Another noninvasive test is vibration-controlled transient elastography, which calculates liver stiffness based on shear wave propagation. The test is self-validating: 10 passes are performed, and the resulting interquartile range indicate the validity of the test. Dr Afdhal pointed out that this test is instantaneous, unlike other modalities. However, acute inflammation, extrahepatic cholestasis, and liver congestion can confound the test [Millonig G et al. J Hepatol. 2010; Arena U et al. Hepatology. 2008; Millonig G et al. Hepatology. 2008]. Failure of transient elastography (TE) occurs in only about 3% of patients, but unreliable results occur in almost 16% and may be due to large variation among interquartile ranges or insufficient number of valid shots [Castéra L et al. Hepatology. 2010].
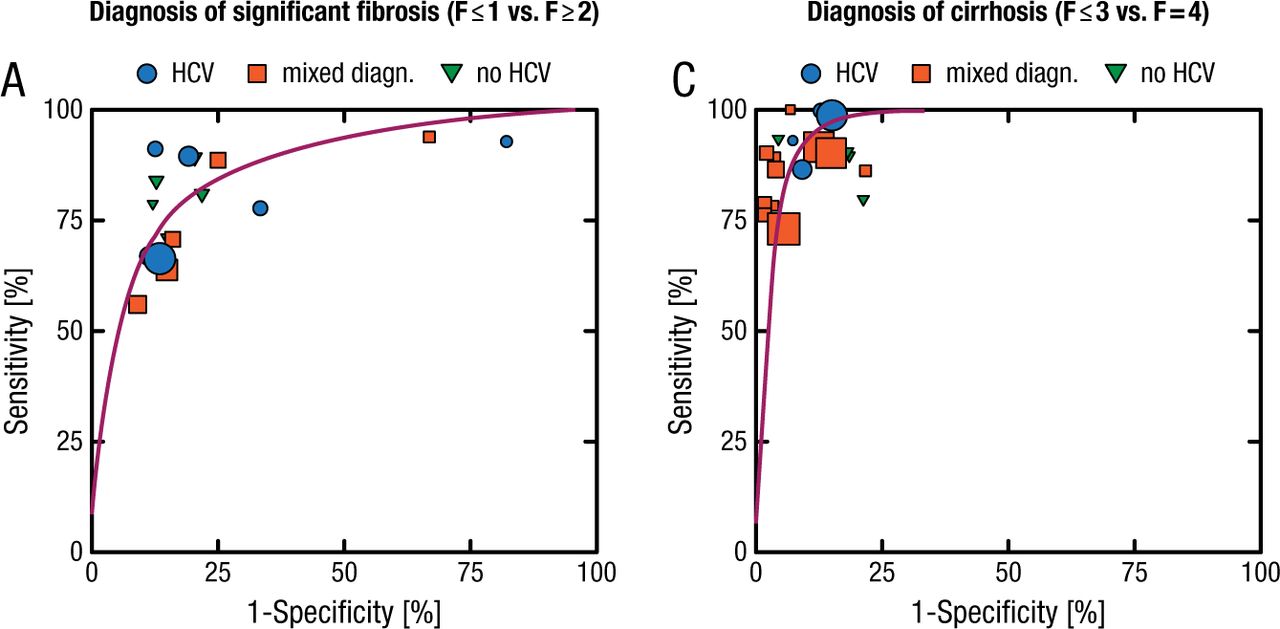
This is particularly a problem in patients who are obese, as the thickness of chest wall fat can impede shear wave penetration. However, an extra-large probe was developed to overcome this limitation, which reduces failure from the 16% in the typical M probe to 1% [Myers RP et al. Hepatology. 2012]. TE performs better than blood tests for identifying significant fibrosis (area under receiving operating characteristic curve [AUROC], 0.84; 95% CI, 0.82 to 0.86) and is excellent for identifying cirrhosis (AUROC, 0.94; 95% CI, 0.93 to 0.95; Figure 1) [Friedrich-Rust M et al. Gastroenterology. 2008]. It also performs well for the middle stages, with about 92% of patients correctly classified [Ganne-Carrié N et al. Hepatology. 2006].
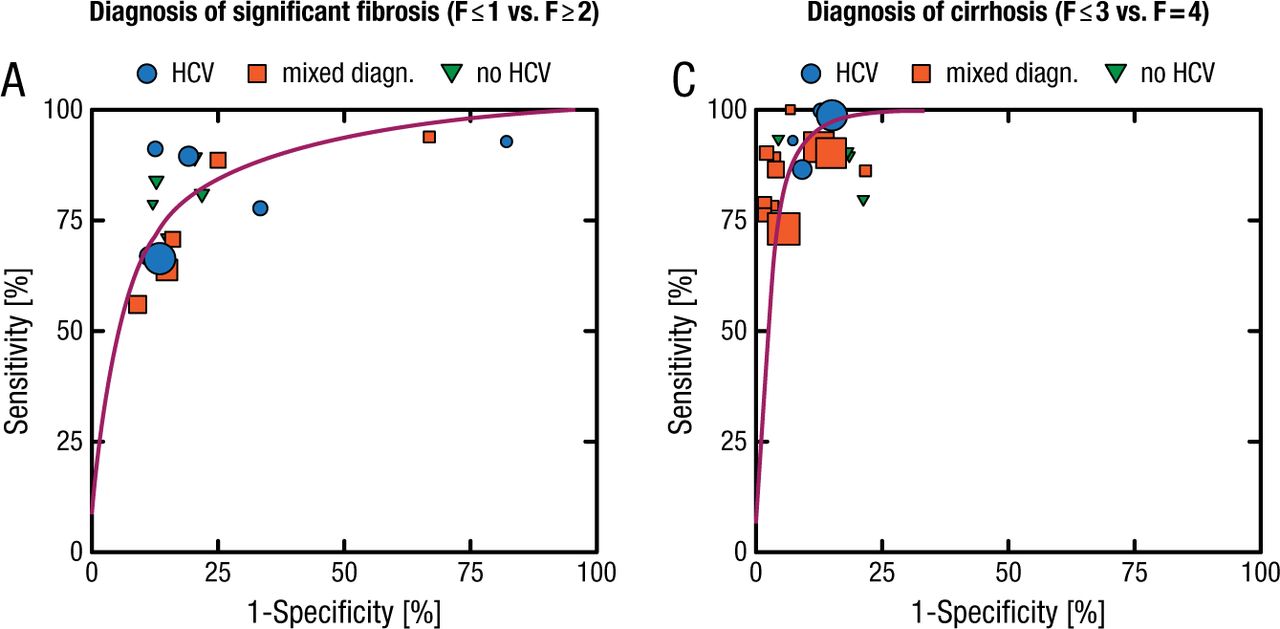
Performance of Transient Elastography vs Blood Tests
(A) SROC for F > 2, (C) F = 4. The size of the dots for 1-specificity and sensitivity of the single studies in the ROC space is derived from the respective sample size. (A–C) •, HCV; ■, mixed diagnosis; ▼, no HCV.
Reprinted from Gastroenterology, Vol. 134, Friedrich-Rust M et al, Performance of Transient Elastography for the Staging of Liver Fibrosis: A Meta-Analysis Pages No. 960-974, Copyright (2008), with permission from AGA Institute.
Other noninvasive tests include novel imaging techniques such as MRE, which performs better than TE, with an AUROC of 0.99 for F ≥ 2 and F = 4 disease [Huwart L et al. Gastroenterology. 2008]. In addition, MRE can identify advanced fibrosis in patients with nonalcoholic fatty liver disease, and 3D MRE is useful for monitoring liver disease as well [Loomba R et al. EASL 2014 (abstract O80)]. Weighted computed tomography mean fibrosis, a 2D ultrasound modality, measures the velocity of shear waves through the liver and has a similar performance as TE [Castéra L. Gastroenterology. 2012; Friedrich-Rust M et al. Radiology. 2009]. It differs from TE in the following: the measurement is in a smaller region of the liver; a regular ultrasound machine can be used; and it can be used in patients who are obese or who have ascites. Its validation is ongoing, and it cannot differentiate among the stages of fibrosis.
In conclusion, the assessment of fibrosis in patients with liver disease is important for diagnosis, staging, and prognosis and for guiding treatment decisions and, in some cases, receiving approval for treatment. Although liver biopsy is the traditional standard of care, TE, MRE, and acoustic radiation force impulse are newer modalities that are able to identify patients in cases where serum biomarker results are inconclusive.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.