

Summary
A flail chest injury occurs when a segment of the thoracic cage is separated from the rest of the chest wall. Such injuries are associated with severe pulmonary restriction; they generally require intubation and mechanical ventilation; and they are associated with high rates of morbidity and mortality. This article discusses flail chest injury data from the National Trauma Databank of North America, the use of open reduction and internal fixation, indications for chest wall repair, as well as the current need for additional trial data.
- Orthopaedic Procedures
- Trauma
- Orthopaedics
- Orthopaedic Procedures
- Trauma
A flail chest injury occurs when a segment of the thoracic cage is separated from the rest of the chest wall. Such injuries are associated with severe pulmonary restriction; they generally require intubation and mechanical ventilation; and they are associated with high rates of morbidity and mortality.
Niloofar Dehghan, MD, St Michael's Hospital, Toronto, Ontario, Canada, presented the results of a retrospective analysis of data from the National Trauma Databank of North America that examined outcomes in 3467 patients admitted to a trauma center with a flail chest injury from 2007 to 2009 [Dehghan N et al. J Trauma Acute Care Surg. 2014]. Outcomes included days on mechanical ventilation, time in the intensive care unit (ICU), length of hospital stay, and rates of pneumonia, sepsis, tracheostomy, chest tube placement, and death. Treatment approach was also an area of interest.
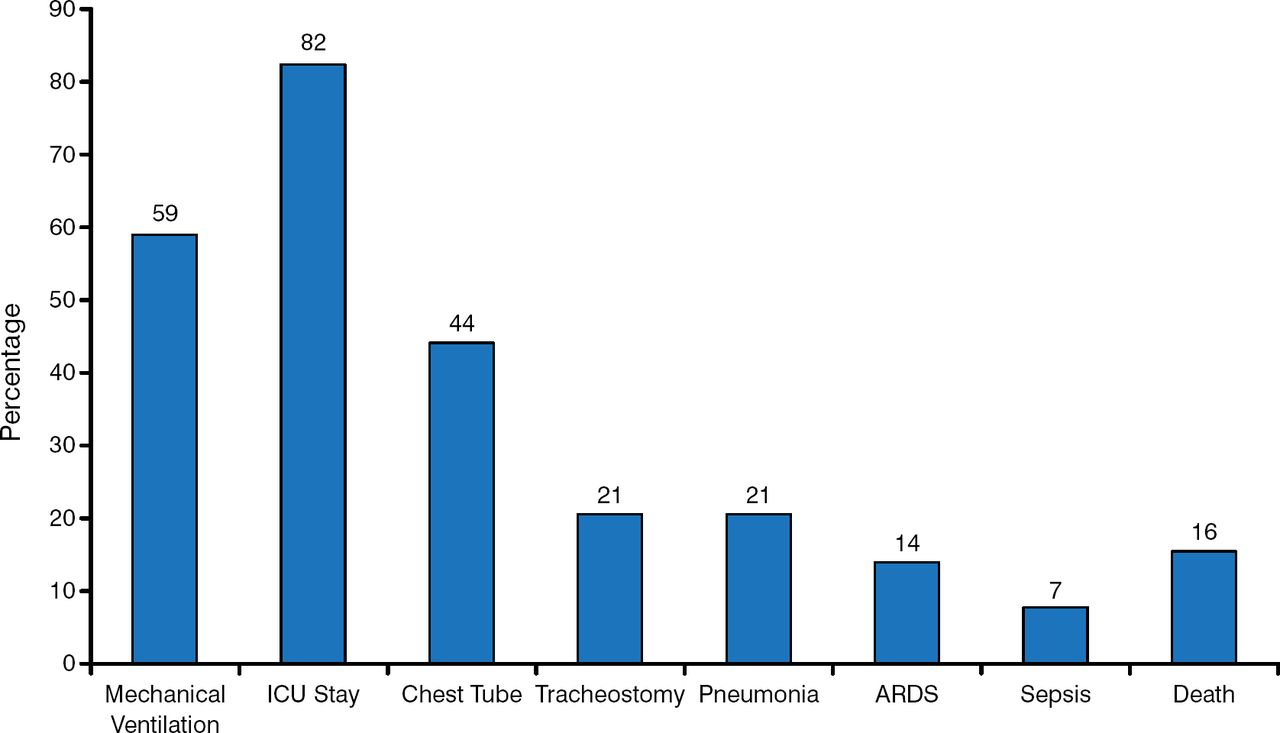
Most patients (82%) were admitted to the ICU (mean stay 11.7 days), and 59% required mechanical ventilation (mean 12.1 days; Figure 1). Patients remained in hospital for a mean of 16.6 days.

Outcomes: Total Population
ARDS, adult respiratory distress syndrome; ICU, intensive care unit.
Adapted from Dehghan N et al. Flail chest injuries: A review of outcomes and treatment practices from the National Trauma Data Bank. J Trauma Acute Care Surg. 2014;76:462–468. With permission from Lippincott Williams & Wilkins.
Patients with concurrent severe head injury (15%) had significantly worse outcomes (P < .05) in every category when compared with those with no head injury. Patients with pulmonary contusions (54%) had a higher need for mechanical ventilation and ICU admission, as well as higher rates of pneumonia and chest tubes.
Only 8% of patients received an epidural catheter for pain control, and very few (0.7%) were treated with open reduction and internal fixation (ORIF). Given the mortality and morbidity in patients with flail chest injuries, alternate methods of treatment need to be investigated, including increased use of epidural catheters for pain and possibly expanded use of surgical fixation.
Interest in surgical fixation for flail chest injuries has been increasing in recent years as a result of new rib-specific implants and recognition of poor outcomes with the current approaches. After conducting a thorough search of the literature, Gerard Slobogean, MD, MPH, University of British Columbia, Vancouver, British Columbia, Canada, believes that there remains insufficient trial evidence to recommend this approach. He noted that only 3 small randomized controlled trials (RCTs) have compared rib fixation with nonsurgical management of flail chest injuries [Marasco SF et al. J Am Coll Surg. 2013; Granetzny A et al. Interact Cardiovasc Thorac Surg. 2005; Tanaka H et al. J Trauma. 2002] and that the remainder of the literature consists of heterogeneous, poorly controlled studies.
Two recent meta-analyses indicate significant benefits with surgical fixation when compared with nonoperative management, in terms of reductions in the duration of mechanical ventilation and ICU stay and decreased mortality, pneumonia, chest deformity, septicemia, and tracheostomy management [Leinicke JA et al. Ann Surg. 2013; Slobogean GP et al. J Am Coll Surg. 2013]. Although these pooled analyses of the existing data generally indicate improved outcomes with surgical fixation, Prof Slobogean cautioned against placing too much reliance on these results, because the data are based mostly on small retrospective studies.
Although the absolute indications for rib fixation remain unclear, it appears that early ORIF shortens ventilator time, improves pulmonary function testing, restores chest wall continuity, and allows patients to return to work faster. Patients treated with ORIF also have less pneumonia, less need for reintubation, decreased home oxygen requirements, and decreased overall costs. In a study reported by Peter L. Althausen, MD, MBA, Reno Orthopaedic Clinic, Reno, Nevada, USA, patients treated with ORIF had better outcomes across all variables. Early operative intervention significantly shortened ICU and hospital stays, as well as days on a ventilator (Table 1).
Effects of Early Operative Intervention for Flail Chest
Other indications suitable for ORIF might include extensive anterolateral flail chest and gross displacement of fractured ribs or a thoracotomy because of an associated intrathoracic injury; alternately, ORIF might be needed for reduction of pain and disability, for revision of malpositioned hardware, and for painful rib nonunion.
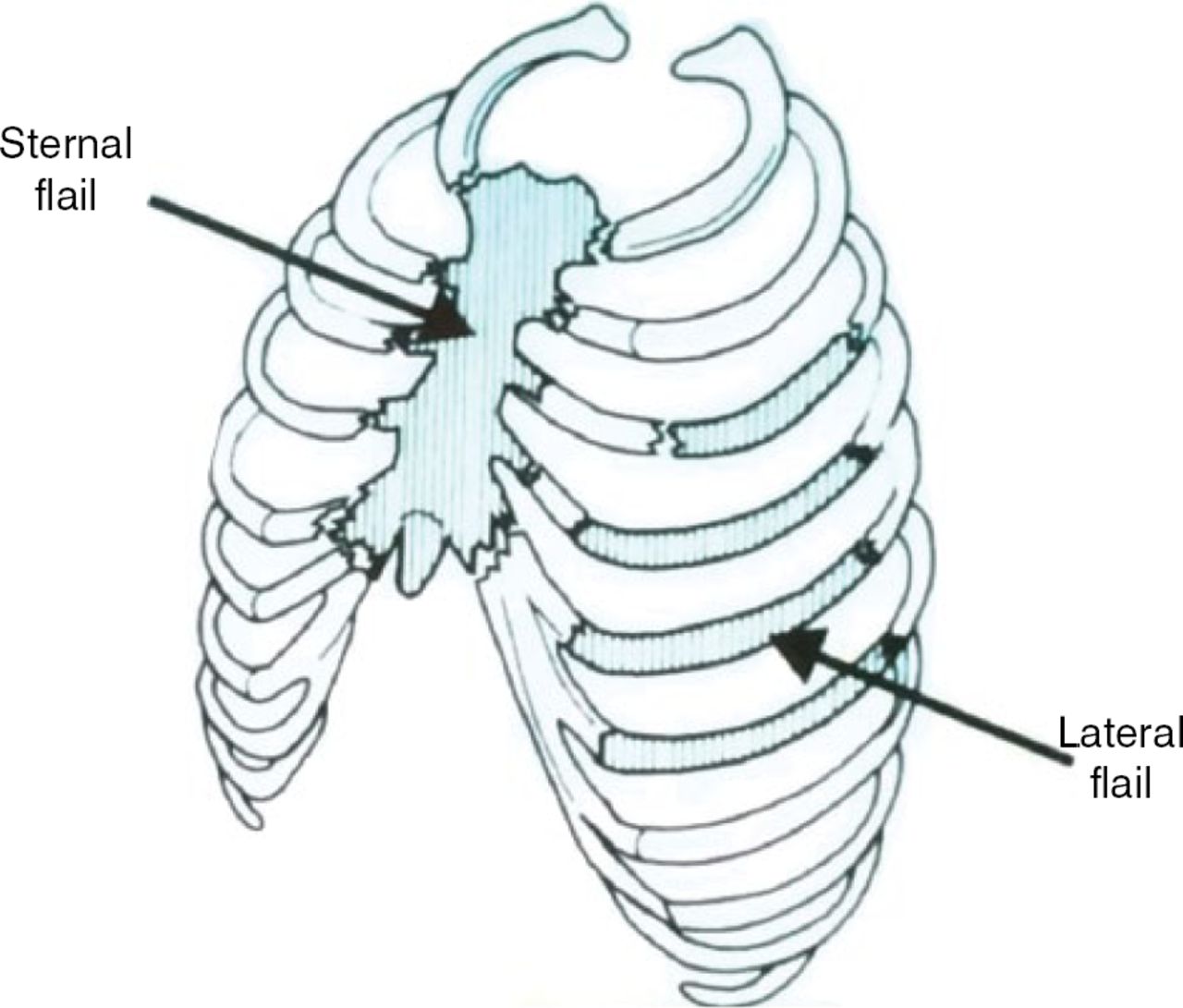
John Mayberry, MD, Saint Alphonsus Regional Medical Center, Boise, Idaho, USA, reviewed indications for chest wall repair along with examples of each. In his opinion, indications for repair include chest wall defect herniation, flail chest (Figure 2) or equivalent, reduction of acute and chronic pain, and nonunion after 4 months. Indications of a true flail chest injury might include persistence of the flail, failure to wean the patient from the ventilator, and continuation of problems with no severe extrathoracic injury.

Diagram of Flail Chest
Reproduced with permission from J Mayberry, MD.
Chest wall implosion is a term used to describe injuries such as fixed deformities of the thoracic cage, multiple segmental rib fractures, and clavicular injury, which can be effectively managed with a posterior paramidline approach without thoracotomy [Solberg BD et al. J Trauma. 2009]. Dr Mayberry believes that these injuries are equivalent to a flail and should be fixed. Although he generally supports surgical fixation, Dr Mayberry believes that careful patient selection and timing of surgery are important for a successful outcome.
Emil H. Schemitsch, MD, St Michael's Hospital, Toronto, Ontario, Canada, discussed the need for more evidence from rib fracture fixation RCTs, preferably prospective randomized multicenter studies with clear inclusion and exclusion criteria and standard treatment arms and outcome measures. While recognizing that such studies are difficult in orthopaedics, he concluded that they are the best evidence for clinical decision making and should thus be the goal.
The impact of unstable chest wall injuries on the health care system is profound (eg, cost of hospital admission and, often, ICU stay; high rates of morbidity and mortality). Prof Schemitsch discussed an ongoing multicenter prospective RCT [NCT01367951] comparing surgical treatment of carefully selected patients with acute unstable chest wall injuries with the current gold standard of nonoperative management. The primary outcome is days free from mechanical ventilation in the first 28 days following injury. The hypothesis of the study is that early surgical fixation of unstable chest wall injuries will significantly improve patient outcomes over conventional, nonsurgical treatment. Patients with flail chest or severe deformity of the chest wall are being enrolled.
In light of the potential for substantial improvement in outcomes with surgical treatment, a well-conceived and well-performed trial has the potential to effect global impact across the multiple health disciplines that treat unstable chest injuries and to provide evidence for substantial health care savings. The potential for a paradigm shift in management also exists.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.