

Summary
A focus on reducing costs of medical care and addressing public and government demand for provider accountability has led to the development and reporting of performance measures for interventional cardiovascular procedures. Professional societies and government agencies are developing data registries and evidence-based performance measures in percutaneous coronary intervention, peripheral intervention, and transcatheter aortic valve replacement.
- data registry
- PCI
- percutaneous coronary intervention
- performance measure
- peripheral artery disease
- risk adjustment
- TAVR
- transcatheter aortic valve replacement
- cardiology & cardiovascular medicine guidelines
- interventional techniques & devices
The American College of Cardiology Foundation and American Heart Association (AHA) performance measures are measures of outcomes, processes, and structure that are based on guideline recommendations that reflect clinical care patterns and are suitable for accountability [Bonow RO et al. J Am Coll Cardiol. 2011]. Performance measures focus on areas with widely accepted evidence and feasible validation. Some performance measures are appropriate for public reporting, while quality metrics are for internal quality improvement. Kalon K. L. Ho, MD, MS, Beth Israel Deaconess Medical Center, Boston, Massachusetts, USA, presented an overview of desirable attributes for performance measures (Table 1).
ACCF/AHA Desirable Attributes of Performance Measures
Performance Measures for Percutaneous Coronary Intervention
Performance measures for percutaneous coronary intervention (PCI) have been published by the American College of Cardiology (ACC), AHA, Society for Cardiovascular Angiography and Interventions, American Medical Association–Convened Physician Consortium for Performance Improvement, and the National Committee for Quality Assurance [Nallamothu BK et al. J Am Coll Cardiol. 2014]. All their performance measures for PCI were also reviewed by Dr Ho and are summarized in Table 2.
2013 ACC/AHA/SCAI/AMA Percutaneous Coronary Intervention Measurement Set
Readmissions Post-PCI Serve as a Performance Measure
Since implementation of the Hospital Readmissions Reduction Program of the Affordable Care Act, there has been a focus on readmissions after PCI as a performance measure. In 2005, the Medicare Payment Advisory Commission identified PCI as 1 of 7 conditions and procedures responsible for most readmissions, with nearly 1 in 6 Medicare patients readmitted within 30 days of PCI. The rate is similar for other payers and varies across hospitals. According to Jeptha P. Curtis, MD, Yale School of Medicine, New Haven, Connecticut, USA, there is evidence that providing better care results in lower readmission rates.
The Centers for Medicare and Medicaid Services (CMS) and the ACC developed unplanned readmissions as a performance measure, using registry data to improve risk adjustment and CMS data to identify outcomes. Implementation began in 2013. Hospitals received detailed information about their risk-standardized readmission rates, and 350 hospitals volunteered to report their outcomes. Although the CMS has not continued to publicly report PCI readmissions, the ACC is considering whether to include PCI readmissions as part of its public reporting effort.
A study of readmissions from 2 academic medical centers showed that about 40% of readmissions after PCI were potentially preventable [Wasfy JH et al. J Am Heart Assoc. 2014]. Furthermore, according to Dr Curtis, readmission rates across a number of medical conditions have declined since outcomes reporting began in 2010.
The Translating Outstanding Performance in PCI study, in collaboration with the ACC, surveyed hospitals performing PCI and found 7 strategies that were strongly associated with lower readmission rates: retaining high-quality staff, regularly meeting with care agencies, having a dedicated unit for PCI patients, adopting new technologies early, including pharmacists in the care of all PCI patients, arranging follow-up appointments before discharge, and withholding the discharge summary from patients and family.
Public Reporting of PCI Mortality
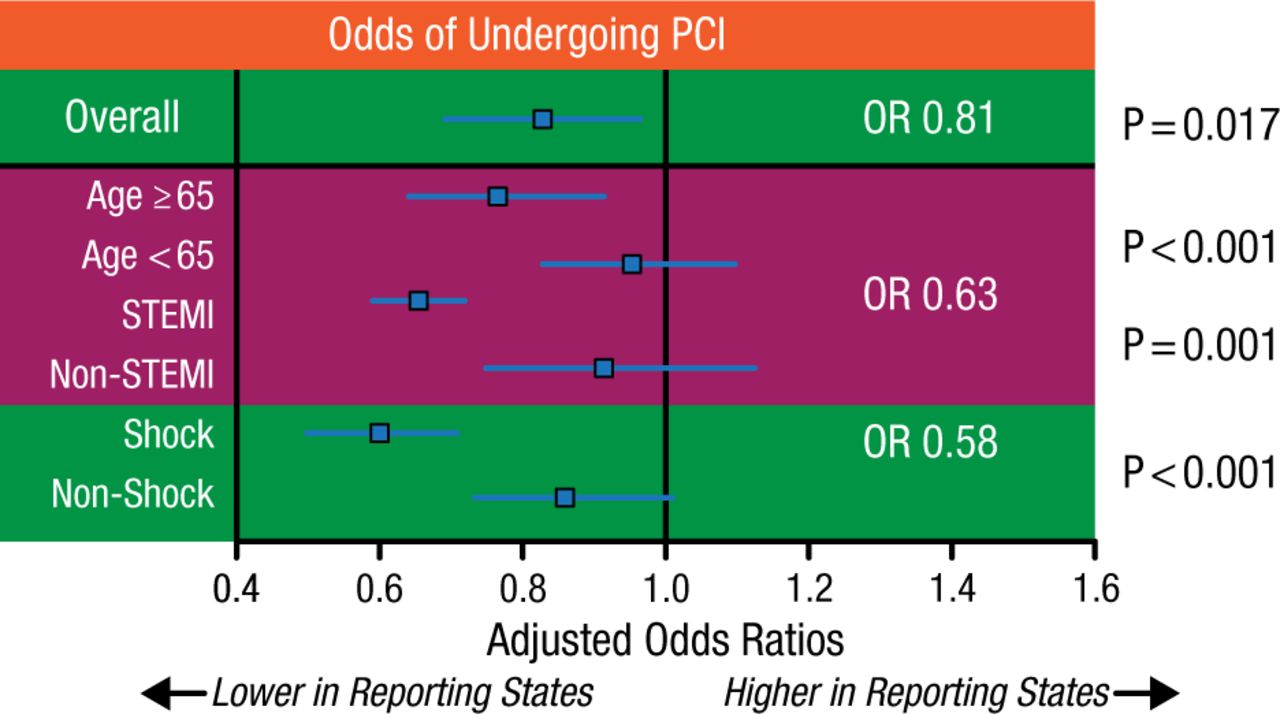
According to Ken Rosenfield, MD, Massachusetts General Hospital, Boston, Massachusetts, USA, mortality after PCI is easy to measure and is an accepted end point in clinical trials and other health care outcomes assessments, with established benchmarks. However, mortality is highly dependent on the complexity of cases and patient risk profiles. Mortality cannot be adequately risk adjusted due to infrequency and high case variability. Given the low frequency of death after PCI and the low volume of operators, 1 or 2 deaths can skew the percentage for individual operators, which might lead to risk avoidance behavior. This was demonstrated in a study showing that public reporting was associated with reduced PCI rates and increased mortality in patients with acute myocardial infarction not selected for PCI (Figure 1) [Waldo SW et al. J Am Coll Cardiol. 2015]. In New York, a public reporting state, selective PCI use led to decreased PCI mortality but increased overall mortality [Apolito RA et al. Am Heart J. 2008].
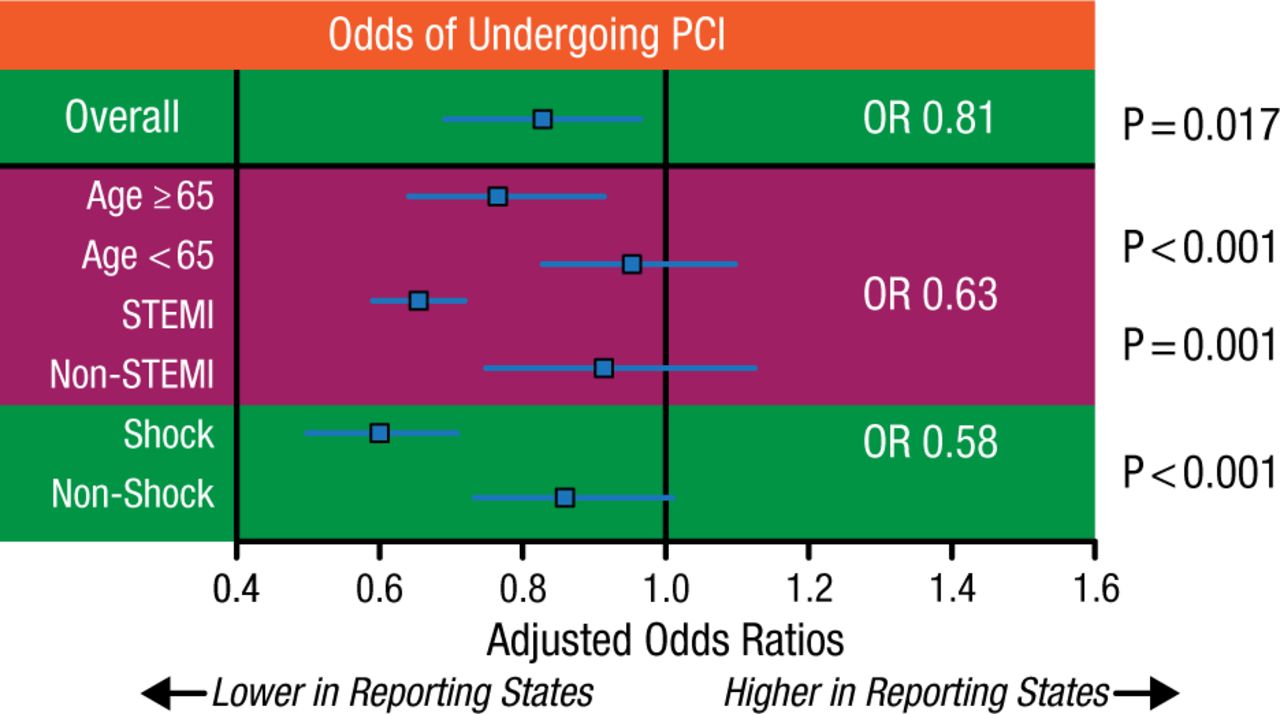
PCI Use in Public Reporting vs Nonreporting States
Adjusted odds of undergoing percutaneous revascularization among patients with AMI was significantly lower in public reporting states than in nonreporting states (p = 0.017). These findings were specifically pronounced among older patients, those with Medicare insurance, and those presenting with STEMI or concomitant cardiac arrest or cardiogenic shock (interaction p < 0.001 for each comparison).
PCI, percutaneous coronary intervention.
Reprinted from J Am Coll Cardiol, Vol 65, Waldo SW et al, Association between public reporting of outcomes with procedural management and mortality for patients with acute myocardial infarction, Pages 1119-1126, Copyright (2015), with permission from American College of Cardiology Foundation.
Physician risk aversion can be mitigated by introducing compassionate-use and exceptional-risk criteria and new variables for risk adjustment, such as surgical ineligibility [Waldo SW et al. Circulation. 2014; Resnic FS et al. J Am Coll Cardiol. 2011]. According to Dr Rosenfield, very high-risk patients perhaps should be excluded from the numerator and denominator of the published report. However, those data should be captured and tracked, and operator reviews should be undertaken to identify issues related to quality and appropriateness. External quality review of outliers can provide context to the statistical report. Finally, Rosenfield supported the concept of independent interfacility peer review of a random sampling of cases to evaluate both quality and appropriateness. Rather than a punitive approach, such a peer review process should be designed to identify potential issues and address them before they become problematic.
Performance Measures for Peripheral Artery Disease
The current most widely used vascular procedure database for outcome analysis is the Vascular Quality Initiative. This initiative involves a collaboration of regional quality groups collecting and analyzing data with the purpose of improving patient care [Vascular Quality Initiative. http://www.vascularqualityinitiative.org/. Accessed May 13, 2015]. The goal of such a database and outcomes analysis is to increase transparency and quality. Mark C. Bates, MD, West Virginia University School of Medicine, Charleston, West Virginia, USA, defined quality as ensuring that the patient has access to the best-quality physicians as documented by objective outcome measures in a facility that is focused on safety and has a patient-centered mind-set.
Performance measures for peripheral artery disease (PAD) are not as well defined as those for PCI, noted Dr Bates. In 2010, several major societies published proposed performance measures for adults with PAD [Olin JW et al. Circulation. 2010]. Dr Bates highlighted critical measures based on these performance measures and the guidelines of the American College of Cardiology Foundation and AHA for the management of PAD (Table 3) [Anderson JL et al. Circulation. 2013].
Critical Measures for Management of Peripheral Artery Disease
The Medicare Evidence Development & Coverage Advisory Committee (MEDCAC) is holding a meeting in July 2015, at which society representatives can provide input on important data for performance measures. MEDCAC is collecting data on whether PAD interventions result in reduced pain, decreased amputation, improved quality of life and functional capacity, wound healing, and decreased cardiovascular events and all-cause mortality and whether there are associated harms to patients.
The Virginia Vascular Study Group collects data and provides feedback for center and physician outliers. According to Dr Bates, the challenge for the future will be mastering “big data” and providing personalized objective recommendations based on data from multiple sources funneling into a central database. This database will house the patient’s genomic fingerprint proteomic data, hospital records, as well as physician assessments, and all outputs will be framed by comparative data from other centers, expert consensus, relevant literature, and expert consensus.
Performance Measures for Transcatheter Aortic Valve Replacement
No specific performance measures for transcatheter aortic valve replacement (TAVR) have been published. However, facilities that perform TAVR are required to submit data to the Society of Thoracic Surgeons and ACC transcatheter valve therapy registry for transcatheter valve replacement and repair procedures. David L. Brown, MD, The Heart Hospital Baylor, Plano, Texas, USA, discussed the evidence for several proposed performance measures for TAVR, including mortality and stroke, renal injury, vascular complications, paravalvular regurgitation, permanent pacemaker implantation, length of stay, economics, and quality of life.
A transcatheter valve therapy registry study reported favorable overall rates of in-hospital mortality (5.5%) and stroke (2.0%) and 30-day mortality (7.6%) and stroke (2.8%) [Mack MJ et al. JAMA. 2013], but 1-year mortality (23.7%) rates were high [Holmes DR Jr et al. JAMA. 2015]. Comparing implantation with Sapien vs CoreValve implantation, several studies found no differences in 1-year mortality and 30-day stroke rates in high-risk and inoperable patients.
Major vascular access site complications are associated with impaired clinical outcomes, increased transfusions, prolonged hospital stay, and increased cost. The percutaneous, transfemoral access route is the preferred and most frequently used access site. The incidence of major vascular access site complications has rapidly declined due to lower profile devices and delivery sheaths, as well as learning experience.
In the PARTNER trial, multivariable predictors of permanent pacemaker implantation after TAVR were as follows: existing right bundle branch block (P < .001), treatment in a registry (P = .025), prosthesis diameter and left ventricular outflow tract diameter (P = .002), and left ventricular end-diastolic diameter (P = .003) [Nazif TM et al. J Am Coll Cardiol Intv. 2015]. Permanent pacemakers increased the risk of hospitalization but not mortality.
From a US societal perspective, TAVR appears to be reasonably cost-effective for both inoperable and high-risk patients, particularly when performed via a transfemoral approach [Reynolds MR et al. J Am Coll Cardiol. 2012]. From a hospital perspective, economics depend heavily on geography and case mix. Ongoing reductions in complications should modestly improve the cost-effectiveness of TAVR. The greatest opportunity lies in maximizing efficiency of care for uncomplicated procedures.
Many challenges remain in the development, implementation, and reporting of performance measures for interventional procedures. Implementation of data registries is ongoing and provides an evidence base for performance measures that accurately reflect the quality of interventional care. Physician risk avoidance is a challenge that may be mitigated by instituting compassionate-use criteria and risk adjustment measures where appropriate.
- © 2015 SAGE Publications
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.