

Summary
Michel Latarjet was the first physician to treat recurrent anterior instability of the shoulder with coracoid transfer and attachment of the conjoined tendon to the anterior glenoid with screws. The procedure, which carries his name, was first performed in 1954 and remains in use today for extra-articular treatment of anterior glenohumeral joint instability. This article discusses recent studies on the use of the Laterjet procedure, arthroscopic approaches for the Latarjet procedure, appropriate use of the Hill-Sachs remplissage procedure, as well as shoulder arthrodesis.
- Orthopaedic Procedures
- Shoulder & Elbow Conditions
- Orthopaedic Procedures
- Shoulder & Elbow Conditions
- Orthopaedics
Michel Latarjet was the first physician to treat recurrent anterior instability of the shoulder with coracoid transfer and attachment of the conjoined tendon to the anterior glenoid with screws, according to Gilles D. Walch, MD, Centre Orthopédique Santy Lyon, France. The procedure, which carries his name, was first performed in 1954 and remains in use today for extra-articular treatment of anterior glenohumeral joint instability.
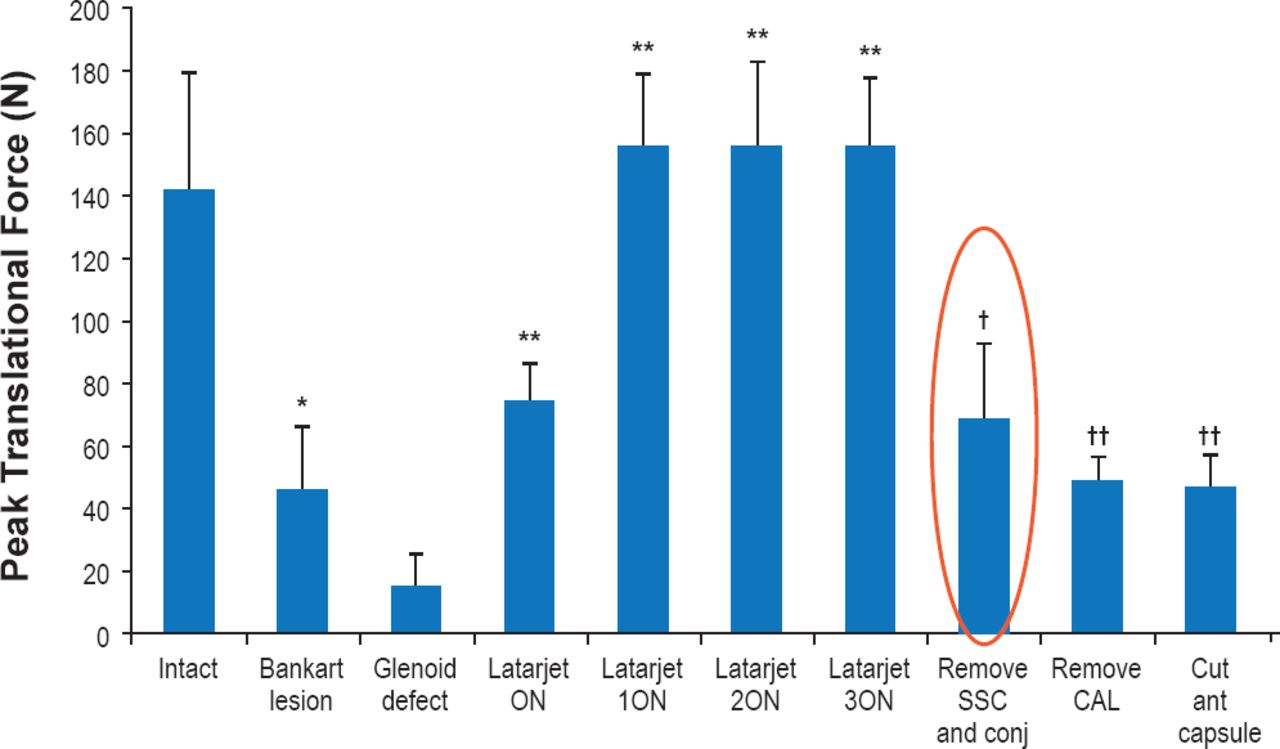
In a recent cadaveric study use of the Laterjet procedure resulted in the return of translational force to levels those seen in the shoulder before a creation of a Bankart lesion or glenoid defect [Yamamoto N et al. J Bone Joint Surg Am 2013]. The sling effect at both the end-range and the mid-range arm positions was the major stabilizing mechanisms of the Latarjet procedure (Figure 1).

Latarjet Procedure Stabilizes the Glenohumeral Joint by the Sling Effect
*p<0.05 compared with the intact condition. **p<0.05 compared with the Bankart lesion. †p<0.05 compared with the Latarjet procedure. ‡p<0.05 compared with the condition after removal of the subscapularis and conjoint tendons. Remove SSC and conj=after removal of the two tendon loads. Remove CAL=after removal of the sutures of the coracoacromial ligament. Cut ant capsule=after release of the attachments of the anterior aspect of the capsule to the glenoid labrum.
Reproduced from Yamamoto N et al. The Stabilizing Mechanism of the Latarjet Procedure: A Cadaveric Study. J Bone Joint Surg Am 2013; 95:1390–1397. With permission from the Journal of Bone and Joint Surgery, Inc.
The primary indications for the use of the Latarjet procedure are recurrent anterior dislocations or subluxations with or without multidirectional hyperlaxity, or primary dislocation in a professional athlete who cannot accept the risk of recurrence. The Latarjet procedure is particularly recommended for atypical and often rare indications such as inferior glenohumeral dislocations (also known as luxatio erecta), humeral avulsion of the glenohumeral ligament (HAG) lesions, instability arthritis, and anterior and post instability seizures. Contraindications for this procedure include unstable painful shoulder, anterior dislocation in the elderly, voluntary laxity, and anterior static laxity. The Latarjet procedure remains a very popular method for treating anterior shoulder instability, with a low rate of recurrence and a high rate of patient satisfaction.
Although safe and reliable, according to Prof. Walch, it is not a universal panacea for all types of anterior laxity or instability. It is not the most appropriate procedure to correct constitutional multidirectional hyperlaxity or for the treatment of painful shoulder in the throwing athlete.
Laurent P. Lafosse, MD, Clinique Général Anncey, Annecy, France, was the first to report the use of an arthroscopic approach for the Bristow-Latarjet procedure in 2007 [Lafosse L et al. J Arthroscopy 2007]. Use of this approach offers the advantages of better visualization, larger access, reduced scarring, reduced postoperative pain, and greater subjective patient satisfaction. It can be converted to an open operation at any stage. Although still somewhat difficult, this technique has improved considerably because of physician experience and new devices. Arthroscopic Latarjet is increasing in popularity as a primary procedure and following Bankart failure.
The first stage of the procedure is joint evaluation and evidence of engaging. In the second step, the intra-articular joint is prepared, an anterior capsulectomy is performed with a shaver, and decortication of subscapularis tendon to facilitate the transfer of the coracoid graft is completed. In the third stage, the coracoid is exposed, debrided, and prepared for osteotomy; the coracoacromial ligament and conjoint tendons are released. The coracoid is harvested in the fourth stage and the anterior subscapularis is prepared and split in the fifth stage. Next, the coracoid is retrieved with a double cannula and placed at the anterior border of the glenoid, then fixed with two screws. The final step is the evaluation of placement arthroscopically.
There have been excellent results with this technique with no recurrence of anterior instability at 6 months. Poor graft placement, nonunion, superior osteolysis leading to massive osteolysis at 6 months and complications can be a concern. Dr. Lafosse recommends arthroscopic Latarjet for patients with recurrent dislocation, glenoid bone loss >10%, and with engaging Hill-Sachs or HAGL lesions. The vast majority of his patients do well, with an incidence of postoperative instability in only 1/63 patients (most recent series). This procedure is recommended to surgeons with good anatomic knowledge, advanced arthroscopic skills, and familiarity with the instrumentation [Lafosse L et al. Orthop Clin North Am 2010].
Arthroscopic Hill-Sachs remplissage, performed in combination with a Bankart repair, is an effective technique in revision of failed instability surgery in a subgroup of patients with a large engaging humeral head bone defect but no substantial glenoid bone loss. Remplissage entails filling the humeral defect with capsule/infraspinatus that prevents anterior engagement. Pascal Boileau, MD, Centre Hospitalier Universitaire Nice, Nice, France, recommends using the Hill-Sachs remplissage procedure when there is an isolated Hill-Sachs lesion without glenoid bone loss or Hills-Sachs lesions associated with glenoid bone loss. The majority of patients have complete healing of the humeral defect (posterior capsulotenodesis). Three steps are performed to complete this procedure in this order: preparation of the Bankart repair in front, Hill-Sachs remplissage in back, and then completion of Bankart repair in front. There is a <100 loss of external rotation with 90% of athletes able to return to full sport activity including those involving overhead activities [Boileau P et al. J Bone Joint Surg Am 2012].
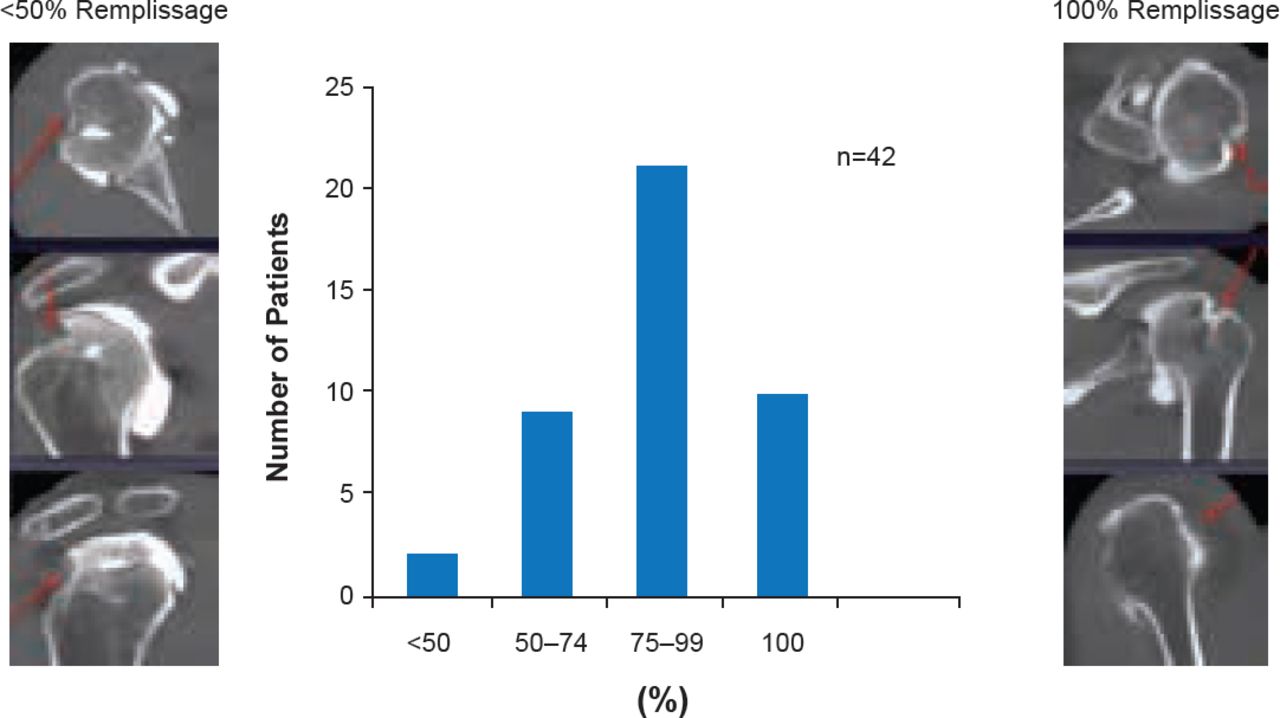
An early retrospective study showed that 94% of patients had good to excellent results and maintained excellent clinical outcomes 4 to 10 years after surgery [Wolf EM et al. Arthroscopy 2004]. In their study, Boileau et al. found that capsule healing in the humeral defect was observed in all patients who underwent postoperative imaging, and thirty-one (74%) had a remplissage of ≥75% (Figure 2) [Boileau P et al. J Bone Joint Surg Am 2012].

Capsule Healing Following Remplissage
Reproduced from Boileau P et al. Anatomical and Functional Results After Arthroscopic Hill-Sachs Remplissage. J Bone Joint Surg Am 2012; 94(7):618–626. With permission from the Journal of Bone and Joint Surgery, Inc.
Prof. Boileau believes this procedure is useful for previously failed glenohumeral instability surgery, but contraindicated for patients with glenoid bone deficiency. Once there is glenoid bone loss, glenoid reconstruction is needed.
Joaquin Sanchez-Sotelo, MD, Mayo Clinic, Rochester, Minnesota, USA, believes shoulder arthrodesis is a good salvage option for patients with persistent instability and irreparable soft-tissue deficiencies. Surgeons should have familiarity with the procedure to perform the operation properly. Beware of these limitations and complications: persistent pain (periscapular), limited motion (trunk-head-shoulder), and complications (fracture, nonunion, hardware removal, malposition, infection). The procedure is best employed in younger patients, who have had multiple surgical attempts. Most of them will have severe soft-tissue deficiency (capsule, subscapularis, deltoid, Ehlers-Danlos), and may have active infection, brachial plexopathy or uncontrolled seizures.
A very early study reported that 86% of patients receiving an arthrodesis believed that they had benefited from the operation, and none of the results deteriorated over the 9.5 months of follow-up. No or mild pain was reported by 74% of the patients [Cofield RH and Briggs BT. J Bone Joint Surg Am 1979]. Complications included nonunions (n=3), fractures (n=10), tenderness over the outer ends of the internal fixation device, which required its removal (n=17) and one infection. In a subset of patients, seven had shoulder instability after 6 years of follow-up. In another study, 57 patients underwent glenohumeral and acromiohumeral arthrodesis [Richards RR et al. J Shoulder Elbow Surg 1993]. The majority (n=54) of shoulders were fused within 10° of the desired position. Three patients required secondary bone grafting. The complication rate was 14%. Patients undergoing the procedure for brachial plexus injury, osteoarthritis, and failed total shoulder arthroplasty reported the highest satisfaction (p=0.0046) as determined by preoperative diagnosis, hand function, and work status. Continued instability was noted in six shoulders.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.