

Summary
The failure rate of hip replacements is an important clinical problem in adult reconstructive orthopedic surgery. Tribocorrosion in the form of articular surface material loss from metal-on-metal bearings and material loss from metal/metal modular junctions is central to the problem. This article provides an update on the clinical impact of tribocorrosion focusing on diagnostic modalities and treatment options.
- Orthopaedic Procedures
- Hip & Knee Conditions
- Orthopaedics
- Orthopaedic Procedures
- Hip & Knee Conditions
The failure rate of hip replacements is an important clinical problem in adult reconstructive orthopedic surgery. Tribocorrosion in the form of articular surface material loss from metal-on-metal (MOM) bearings and material loss from metal/metal modular junctions is central to the problem. In this symposium, experts provided an update on the clinical impact of tribocorrosion focusing on diagnostic modalities and treatment options.
WHAT DO IMPLANT RETRIEVAL STUDIES TELL US?
Alister Hart, MD, Royal National Orthopaedic Hospital, Stanmore and University College, London, United Kingdom, discussed the work of the London Implant Retrieval Center (LIRC).
The LIRC has collected over 5000 failed MOM hip components from 22 countries. Data about these implants are being analyzed to assess the causes of failure, the factors that influence wear, and how the wear occurs. About 1% of the components show obvious evidence of component size mismatch [Whittaker RK et al. J Arthroplasty 2014]. By analyzing radiographs, LIRC was able to identify the cause of the high revision rate for the Durom device as cup loosening caused by a consistent 20 micron flattening of the femoral head that was likely due to poor design [Matties AK et al. Hip Int 2011]. They were also able to determine that differences in design make the Articular Surface Replacement prosthesis more susceptible to suboptimal positioning than the Birmingham Hip Resurfacing prosthesis [Underwood R et al. J Bone Joint Surg Br 2011]. The LIRC is working on linking to registry data to provide even more robust data to improve these devices.
Corrosion of modular junctions can lead to component fracture and the resulting metal ions and particulate debris can profoundly affect periprosthetic tissues and can disseminate systemically. Robert M. Urban, MD, Rush University Medical Center, Chicago, Illinois, USA, discussed how implant retrieval studies of modular junctions are enhancing our understanding of failure in these devices.
Surface defects such as pitting and cracking reduce the fatigue life of the alloy and can lead to catastrophic failure of the neck, noted Dr. Urban, while corrosion generates particulate debris that can contribute to aseptic loosening of the device. In one study of 58 titanium-alloy on titanium-alloy neck-stem junctions retrieved after a median of 15 months, Dr. Urban and colleagues noted that >50% had “moderate” to “marked” corrosion that increased with time, and that corrosion of cobalt chromium (CoCr) modular junctions can occur whether the alloy is mated with itself, titanium, or ceramic. An analysis of 153 CoCr head/titanium-alloy neck combinations that had been in use for 23 months showed 25% to have moderate to marked corrosion in the head and 14% in the neck. In a study of 173 CoCr head/neck combinations moderate to marked corrosion was noted in 16% of heads and 15% of necks. Other corrosion-related issues include chromium phosphate particles that can contribute to device wear and loosening, adverse local tissue reactions (ALTRs) as they always lead to necrosis, and although rare, systemic dissemination of metal ions and particles to organs and bone marrow.
Dr. Urban suggested that there is a need to minimize the generation of ionic and particulate corrosion products, better understand fretting corrosion, and develop strategies to mitigate corrosion.
The differential diagnosis in patients with painful MOM total hip arthroplasty (THA) can be complex and includes a variety of factors intrinsic and extrinsic to the hip [Kwon YM et al. J Arthroplasty 2012]. Young-Min Kwon, MD, PhD, Massachusetts General Hospital, Boston, Massachusetts, USA, reviewed the consensus paper developed by the American Association of Hip and Knee Surgeons, the American Academy of Orthopaedic Surgeons (AAOS), and the Hip Society, which outlines a systematic approach to the assessment and management of these patients (Table 1) [Kwon YM et al. J Bone Joint Surg 2014].
Systematic Risk Stratification
The consensus paper recognizes the need for an individualized approach to each patient and acknowledges that there is insufficient high-quality evidence to develop formal guidelines. Details on each of the classifications are available on the AAOS website at http://www.aaos.org/about/papers/advistmt/1035.asp.
ADVERSE LOCAL TISSUE REACTIONS
The diagnosis of infection in hip and knee replacement can be complicated by ALTRs, which can mimic purulence and cell counts that are not always reliable. Craig J. Della Valle, MD, Rush University Medical Center, Chicago, Illinois, USA, discussed the results of a study examining the utility of erythrocyte sedimentation rate (ESR)/C-reactive protein (CRP) followed by synovial fluid white blood cell (WBC) count and differential to distinguish ALTRs from infection. They examined 150 patients (mean age at surgery 59.2 years; 48% women) with hips having an MOM bearing, a corrosion reaction, or nonarticular surface wear. The mean time to revision was 56.3 months. Nineteen hips were determined to have deep infection; 131 had aseptic revisions. In about one third of cases, an automated synovial WBC count was found to be unreliable. The rate of false-positives was ∼10%. Cases with infection had significantly higher ESR (p=0.0001) and CRP (p=0.0432) than cases without infection and were similar to the current standards, indicating that they are good first-line screening tools. The difference in synovial fluid WBC count and differential were also significantly higher among patients with infection (p=0.0432 and p<0.0001, respectively). Optimum thresholds to differentiate infection from ALTR are shown in Table 2.
Optimum Thresholds to Differentiate Infection From ALTR
Dr. Della Valle concluded that the evaluation used to assess for infection is useful; however, given the 10% rate of false-positives for synovial WBC it should only be relied on if a manual count is done or if a differential can be performed.
Although we have known that modular junctions are a potential source of metal release through corrosion for some time, only recently has this been widely recognized as a potential cause of ALTRs. H. John Cooper, MD, Lenox Hill Hospital, New York, New York, USA, discussed ALTRs associated with modular tribocorrosion.
About 70% to 80% of all cases of ALTR are among women. The etiology of the preponderance among women is unclear. Dr. Cooper suggested that it may be due to an immunologic mechanism that is different in women. In general, symptoms can present as early as 0.7 years (mean, 3.9 years) after THA for head/neck corrosion or 5 months (mean, 7.9 months) after THA for neck/body corrosion. Most patients present with pain in the groin but other areas such as the buttock, trochanteric, or thigh may be affected. Many patients have swelling/fluid collection and/or muscle weakness, with a resultant limp; some report recurrent instability without pain as their only symptom.
ALTRs have only been reported in association with CoCr modular junctions; however, they are not unique to any one brand or device nor are they confined to any one head size. Dr. Cooper stressed the importance of a diagnostic workup to differentiate ALTR from infection. Radiographs should be taken in all cases of patients who present with pain. In 5% to 10% of patients some resorption of the calcar can be seen. As this is related to the presence of a tissue or fluid mass in and around the hip joint it should raise the possibility of an ALTR. Advanced 3D imaging should also be performed. Because cobalt and chromium levels are almost always elevated in patients with taper corrosion a serum metal level workup is important.
In patients with head/neck corrosion, Dr. Cooper recommends removing and cleaning the head, and, as long as there has been no structural compromise to the taper junction, replacing it to avoid the morbidity of removing a well-fixed femoral stem. Changing to a ceramic head can remove a potential source of cobalt debris and may lower the risk of corrosion [Huot Carlson JC et al. J Arthroplasty 2012]. Revision surgery for neck/body corrosion usually requires removal of the entire stem. Clinical results are good after revision for head/neck taper corrosion. Patients report less pain, and metal levels generally return to normal within the first year; however, there is a high complication rate that includes peroneal nerve palsy, periprosthetic joint infection, and recurrent instability.
ELEVATED METAL ION LEVELS
Co and Cr are essential trace elements for normal human health. They are present in many foods, contribute to many key metabolic pathways, and they make strong, hard-wearing bearings. However in excess they can be toxic. J. Mark Wilkinson, MD, University of Sheffield, Sheffield, United Kingdom, discussed the systemic effects of elevated metal ion levels.
Under normal CoCr MOM bearing, the ion levels are low and reach their peak ∼1 year post surgery at a level that is ∼20 times normally seen physiologically. Long-term studies show metal levels of ∼1 to 2.5 μg/L. In contrast, an abnormally functioning bearing or taper may produce much higher metal levels that, on occasion, have exceeded 300 μg/L systemically.
Most of the literature on the systemic effects of metal ions comes from case reports. Prof. Wilkinson discussed an unpublished systematic review he conducted in conjunction with the United Kingdom National Poisons Centre to search for toxicity attributed to metal implants [Bradberry SM et al. Clin Toxicol. Under review]. Data were obtained from Medline from 1950 and Embase from 1980 through February 28, 2014. A total of 279 unique references were identified; however, only 25 papers reported original data and only 18 unique cases were identified. Ten of the 18 cases were due to metal release resulting from replacement of a fractured ceramic bearing with a Co/Cr head. The remaining eight were associated with large-diameter MOM bearings, most of which were stemmed prostheses. Cobalt levels in the all ceramic revision patients were ≥300 μg/L compared with the MOM primary patients in whom only a few patients reached that level. Neuro-ocular toxicity was most common symptom (15 of 18 patients), followed by cardiotoxicity (11/18), and hypothyroidism (9/18). Removal of the prosthesis generally led to symptom improvement.
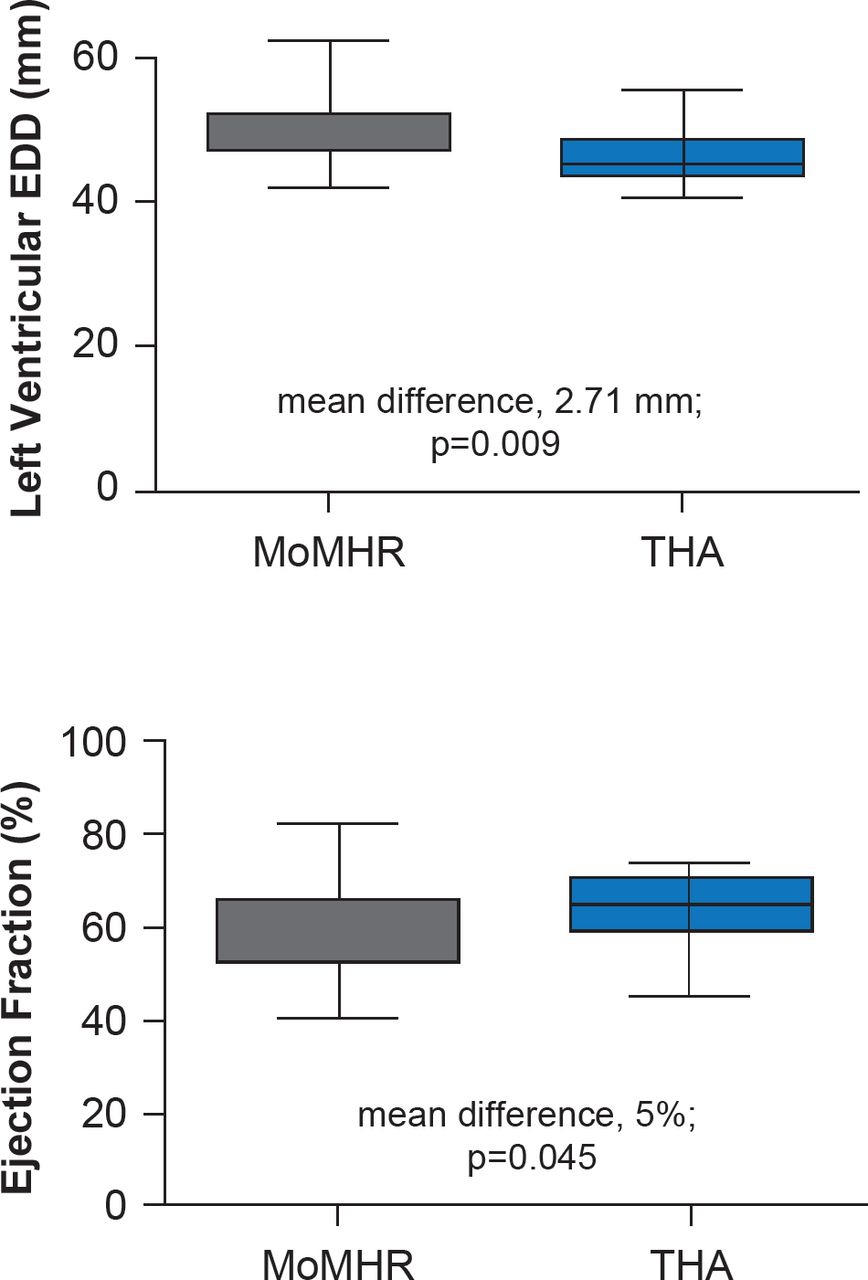
A recent cross-sectional study that examined the cumulative effects of chronic low-dose metal exposure in 35 patients with normal functioning MOM bearings compared with 35 patients with THA showed potentially positive effects on bone mass but possibly injurious effects on left ventricular function in the MOM group (Figure 1) [Prentice JR et al. PLoS One 2013]. MRI studies in these patients showed some differences in gray matter in the occipital areas, near the auditory areas and around the basal ganglia [Clark MJ et al. Am J Neuroradiol 2014. In press]; however, no hearing or vision effects were noted in the MOM group [Prentice JR at al. PLoS One 2014].

Cardiac Function
EDD=end-diastolic diameter; MOMHR=metal-on-metal hip resurfacing; THA=total hip arthroplasty.
Source: Prentice JR et al. PLoS One 2014.
Prof. Wilkinson concluded that high-level exposure with clinical deficit is rare but more likely to occur in patients with previous ceramic revision. Although low-level chronic exposure is common, the effects are subtle and is unlikely to lead to clinical toxicity at Co levels < 100 μg/L.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.