

Summary
Preliminary data indicate that repetitive transcranial magnetic stimulation (rTMS) is superior to a sham treatment for patients with generalized anxiety disorder (GAD). This article presents the results of an ongoing randomized controlled trial to assess the efficacy of rTMS versus sham treatment for patients with moderate to severe GAD.
- Anxiety Disorders
- Psychiatry Clinical Trials
- Psychiatry & Psychology
Preliminary data indicate that repetitive transcranial magnetic stimulation (rTMS) is superior to a sham treatment for patients with generalized anxiety disorder (GAD). Gretchen J. Diefenbach, PhD, Institute of Living at Hartford Hospital, Hartford, Connecticut, USA, presented the results of an ongoing randomized controlled trial to assess the efficacy of rTMS versus sham treatment for patients with moderate to severe GAD.
In total, 32 patients were enrolled in the study. All patients were at least 18 years of age, with a principal or a coprincipal diagnosis of moderate to severe GAD. Patients were excluded if they had a brain trauma or a disorder, a medication change within 3 months of the trial, a serious or unstable medical illness, a substance use disorder within 6 months of the trial, a lifetime diagnosis of select psychological diseases (bipolar disease, developmental disorder, obsessive-compulsive disorder, or psychosis), or current posttraumatic stress disorder; were on medications that increased the risk of seizure due to rTMS; were undergoing concurrent psychotherapy; were too unstable to participate; or had any contraindication to magnetic resonance imaging (MRI).
The patients treated by rTMS were treated with low frequency (1 Hz) to the dorsolateral prefrontal cortex (DLPFC) 5 days a week for 6 weeks, which included 900 pulses per session for 270,000 pulses in total.
The primary outcome was an improvement in anxiety as measured by the Hamilton Anxiety Rating Scale (HAM-A), with a response indicated by 50% more improvement and a remitter indicated by a post score of <8.
Patients were assessed prior to treatment, weekly during treatment, after treatment, and at 3-month follow-up. Adverse events were checked daily during the first week, and weekly thereafter. Functional MRI (fMRI) was performed prior to and after treatment. Preliminary results from fMRI assessments were presented by Assaf and colleagues and showed that there was a significant correlation between symptom changes and changes in neural activation at the right DLPFC, such that symptom improvement was associated with increased neural activation [Assaf MA et al. Presented at the Annual Meeting of the Society of Biological Psychiatry, New York, New York (May 2014)].
Of the 32 patients enrolled, 12 were randomized to active rTMS and 12 to sham. Of these, 7 of 12 in the rTMS group and 8 of 12 in the sham group completed treatment, and 5 and 6, respectively, completed 3-month follow-up.
Dr. Diefenbach presented the results on only the patients who completed treatment so far, and she emphasized that the study is ongoing.
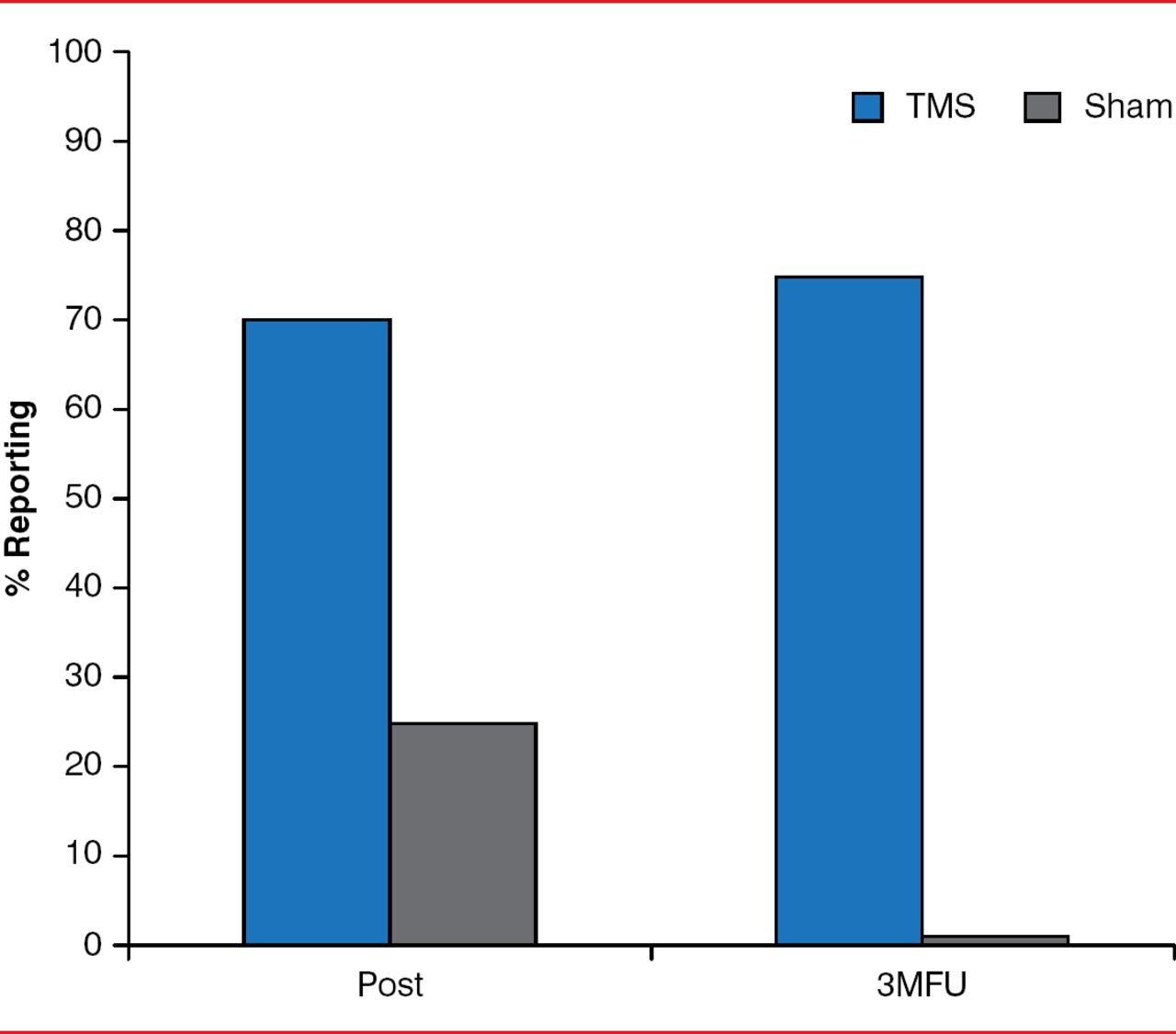
Based on the HAM-A scale, the study found that >70% of patients in the TMS group were categorized as responders after treatment compared with 25% in the sham group (Figure 1). At 3-month follow-up, 80% of the rTMS patients and 0% of the sham patients were responders.

Responders Based on the HAM-A Scale
3MFU=3-month follow-up; HAM-A=Hamilton Anxiety Rating Scale; TMS=transcranial magnetic stimulation.
Reproduced with permission from GJ Diefenbach, PhD.
The study also found that 43% of the patients in the rTMS group and 13% in the sham group were categorized as remitters after treatment, with 80% and 0%, respectively, considered remitters at 3-month follow-up.
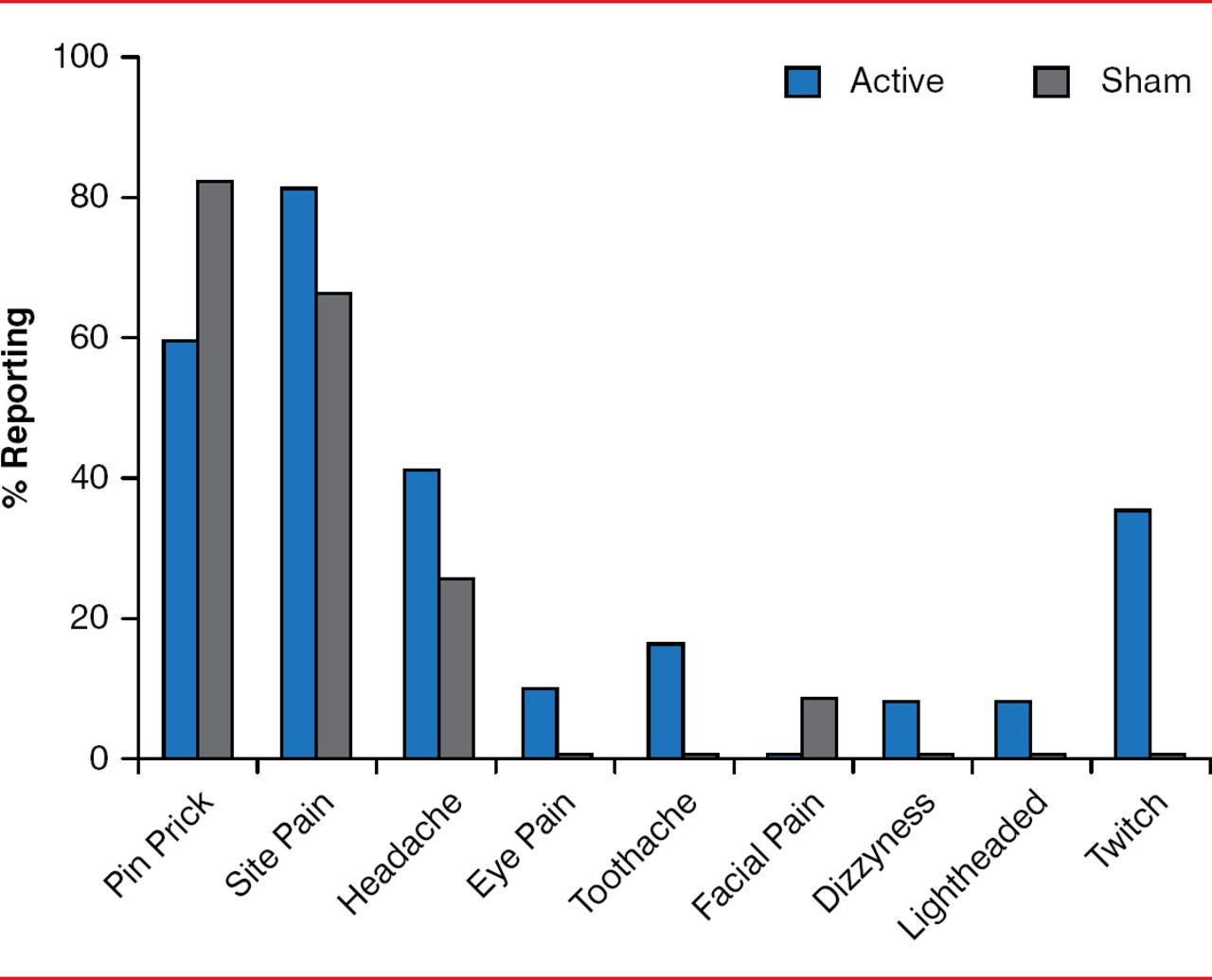
Overall, the incidence of adverse events was similar between the two groups, said Dr. Diefenbach, except for an increased incidence in eye twitch in the rTMS group (Figure 2).

Adverse Events
Reproduced with permission from GJ Diefenbach, PhD.
One serious adverse event occurred in a patient who was hospitalized for chest pain and was diagnosed with coronary vasospasm unrelated to the study procedure or device. No seizures were reported.
Dr. Diefenbach emphasized the importance of further exploring different treatment parameters, saying that one of the main challenges of the trial was the treatment schedule, to which many patients could not commit.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.