

Summary
This article presents data from a meta-analysis of randomized controlled trials in transcranial magnetic stimulation (TMS) among depressed patients. The results showed that TMS appears effective in treating anxiety symptoms in patients with depression.
- Mood Disorders
- Anxiety Disorders
- Psychiatry Clinical Trials
- Psychiatry
- Mood Disorders
- Anxiety Disorders
- Psychiatry Clinical Trials
Gretchen J. Diefenbach, PhD, Institute of Living at Hartford Hospital, Hartford, Connecticut, USA, presented data from a meta-analysis of randomized controlled trials (RCTs) in transcranial magnetic stimulation (TMS) among depressed patients. The results showed that TMS appears effective in treating anxiety symptoms in patients with depression.
Although studies have increasingly shown evidence for the efficacy of TMS among patients with depression [Slotema CW et al. J Clin Psychiatry 2010; Schutter DJ. Psychol Med 2009], its anxiolytic effect is poorly documented. However, based on the comorbidity of anxiety and depression, this is an important area to investigate. Additionally, among patients with depression who also have anxiety, its symptoms tend to be more severe and also maybe more treatment resistant.
To further investigate this, Dr. Diefenbach and colleagues conducted a meta-analysis of data from RCTs to establish the pooled anxiolytic treatment effect of TMS among depressed patients. They used the Hamilton Depression Rating Scale as an outcome measure to assess anxiety symptom change, specifically using the anxiety/somatization subscale, which comprises 6 items: anxiety (psychic), anxiety (somatic), somatic symptoms (gastrointestinal), somatic symptoms (general), hypochondriasis, and insight.
They performed a literature search of the Scopus, Medline, and PsycINFO databases, using search terms including transcranial magnetic stimulation or TMS or rTMS; controlled trial or sham or RCT; and depression or depressive disorder or MDD, which identified 634 articles through June 2013. To be included in the meta-analysis, studies were required to be an RCT comparing TMS versus sham that treated depressive symptoms as the primary target, with TMS targeting the dorsolateral prefrontal cortex. They also had to comprise an adult sample with major depressive disorder, register the Hamilton Depression Rating Scale, and be published in English. Of these 634 articles, 64 met the inclusion criteria, but none of the publications contained all the relevant data, so authors were contacted directly. Complete data were subsequently acquired for 12 studies. Of the combined study participants (n=709), 395 received TMS and 314 received sham treatment.
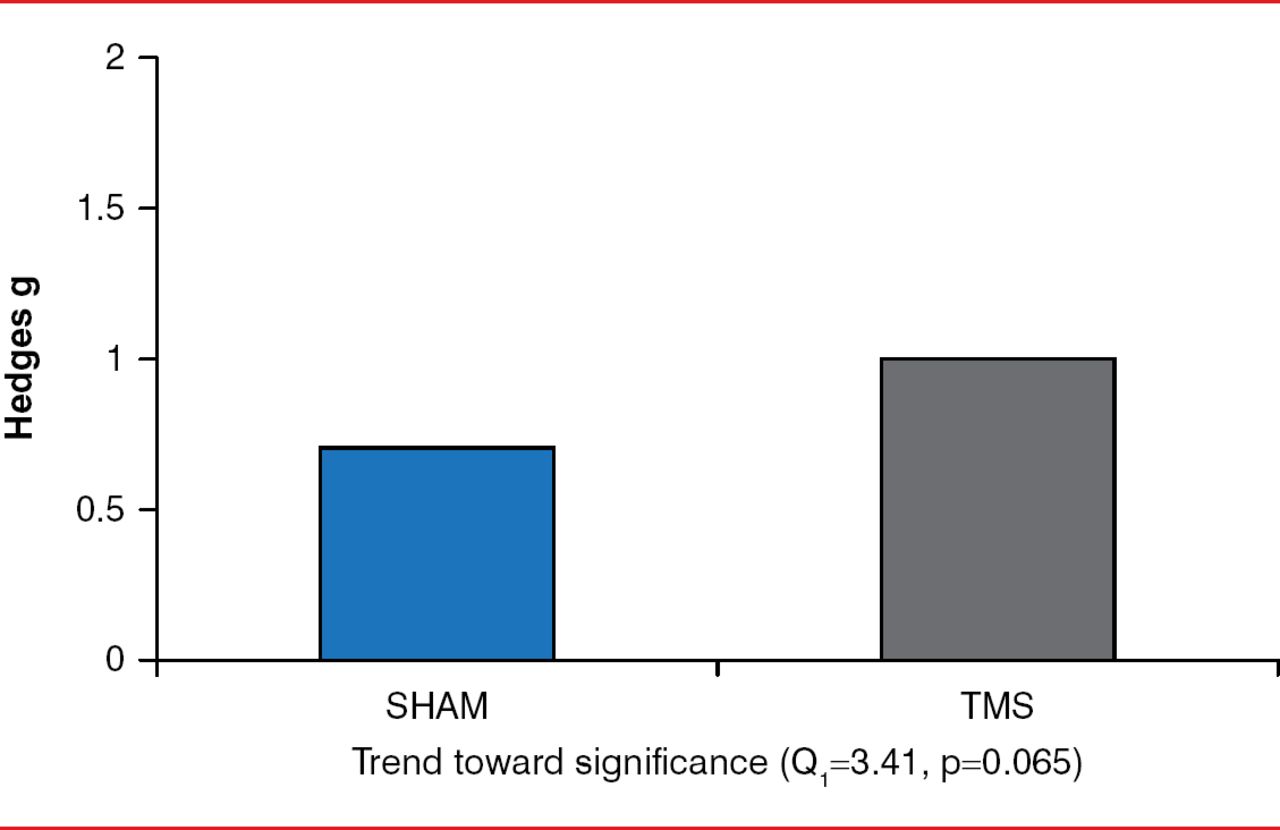
There was no significant difference in mean pretreatment scores between the 2 groups. The statistics associated with the null result are as follows: rTMS group mean score, 7.56; sham group mean score, 7.48; t(25)=0.15; p=0.88. However, analysis of the in-group pooled treatment effect showed a moderate treatment effect for sham and a large treatment effect for TMS, with the difference between them trending toward statistical significance (p=0.065; Figure 1). There was also a moderate but significant difference (p<0.001) in posttreatment between-group effect sizes. Patients who received TMS reported lower anxiety somatization subscale scores than those who received sham. The large fail-safe number (n=102) suggests that these meta-analytic findings are robust.

Posttreatment Between-Group Effect
TMS=transcranial magnetic Stimulation.
Reproduced with permission from GJ Diefenbach, PhD.
The researchers did not pursue analyses of treatment moderators, since there was no significant difference (p=0.56) in between-study heterogeneity, which implied that the results were generally uniform across the different studies.
The results of this meta-analysis indicate that TMS is superior to sham for treating anxiety symptoms in patients with depression, and Dr. Diefenbach concluded that it is important to consider expanding TMS treatment to anxiety disorders. She also indicated that it is important for investigators in future studies to include anxiety assessments in their TMS research, to evaluate changes in individual symptoms, response rates, and anxious depression status.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.