

Summary
The results of the Gulf Acute Heart Failure Registry [GulfCARE; NCT01467973] showed that patients in the Middle East who are diagnosed with acute heart failure are younger than their Western counterparts, have a higher rate of diabetes mellitus, and lower rate of atrial fibrillation. Mortality rates are close to those reported in Western studies; however, this should be re-evaluated in light of the younger age of Middle Eastern patients.
- Cardiology Clinical Trials
- Heart Failure
- Prevention & Screening
- Cardiology & Cardiovascular Medicine
- Cardiology Clinical Trials
- Heart Failure
- Prevention & Screening
The results of the Gulf Acute Heart Failure Registry [GulfCARE; NCT01467973], reported by Kadhim Jaffer Sulaiman, MD, Royal Hospital, Muscat, Oman, showed that patients in the Middle East who are diagnosed with acute heart failure (AHF) are younger than their Western counterparts, have a higher rate of diabetes mellitus (DM), and lower rate of atrial fibrillation (AF). Mortality rates are close to those reported in Western studies; however, this should be re-evaluated in light of the younger age of Middle Eastern patients.
GulfCARE is a prospective registry of patients with AHF who were admitted to participating hospitals between February 14 and November 13, 2012, and who were followed up with at 3 and 12 months. The primary objective of the study was to describe the characteristics, management, and outcomes of hospitalized patients with AHF in the Middle East. GulfCARE comprises 5005 patients (63% men) recruited from 7 Middle Eastern countries. Incident HF was observed in about 45% of patients; the remaining 55% had acute decompensated heart failure (ADHF). HF with reduced ejection fraction (HFrEF) was diagnosed in 69%, with EF preserved in the remaining 31% of patients.
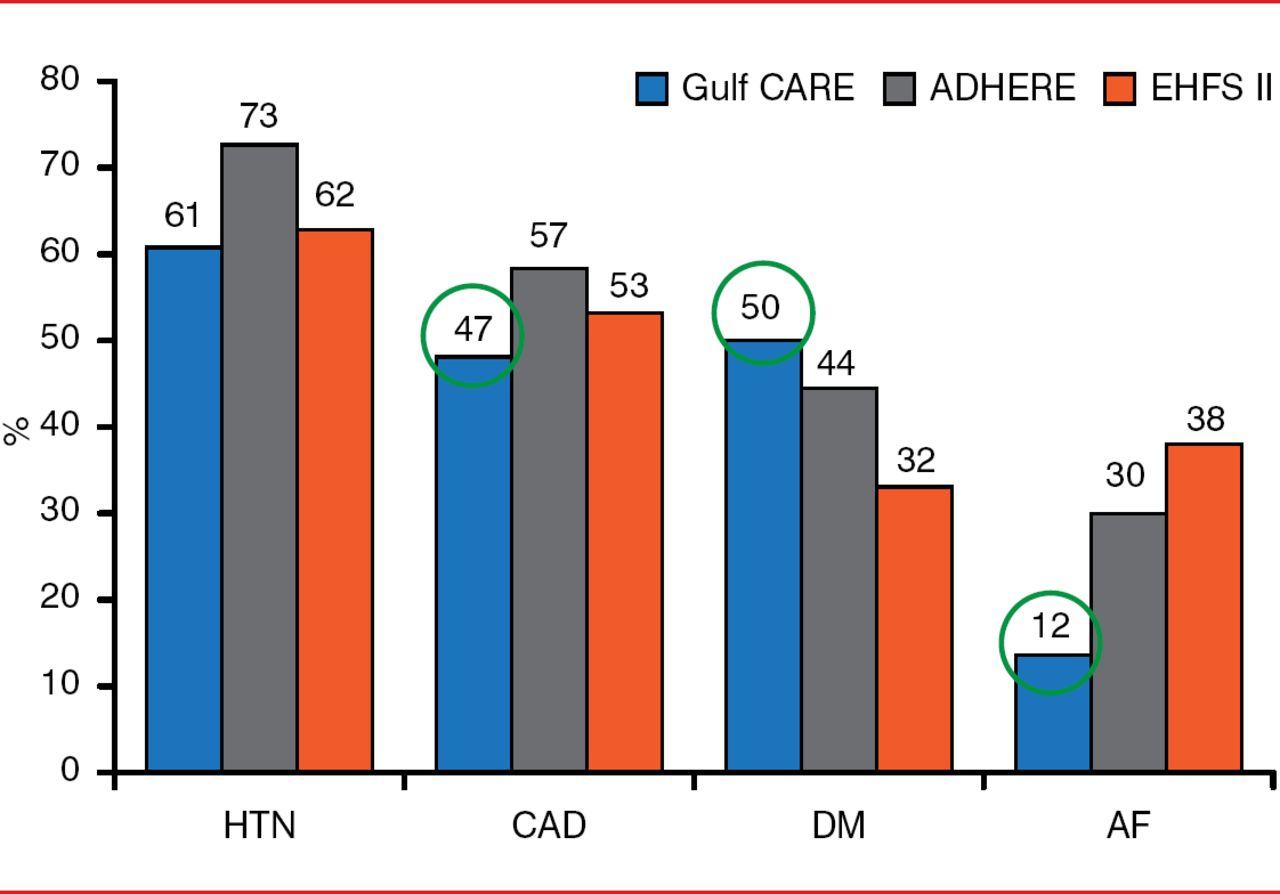
Patients in this study were younger than AHF patients participating in Western studies (mean age, 59 years vs 70 to 73 years, respectively) [Gheorghiade M et al. JAMA 2006; Nieminen MS et al. Eur Heart J 2006; Adams KF et al. Am Heart J 2005]. About half of GulfCARE participants (47%) had coronary artery disease (CAD), and 12% had AF. Hypertension was present in 61% of patients, 50% had DM, and 36% had hyperlipidemia. Compared with the populations in Western AHF studies, patients in the GulfCARE study had lower rates of CAD and AF but higher rates of DM (Figure 1). About 75% of patients in GulfCARE had New York Heart Association Class III or IV at admission.

Medical History
AF=atrial fibrillation; CAD=coronary artery disease; DM=diabetes mellitus; HTN=hypertension.
ADHERE: Adams KF et al. Am Heart J 2005; EHFS II: Nieminen MS et al. Eur Heart J 2006.
Reproduced with permission from Sulaimab KJ, MD.
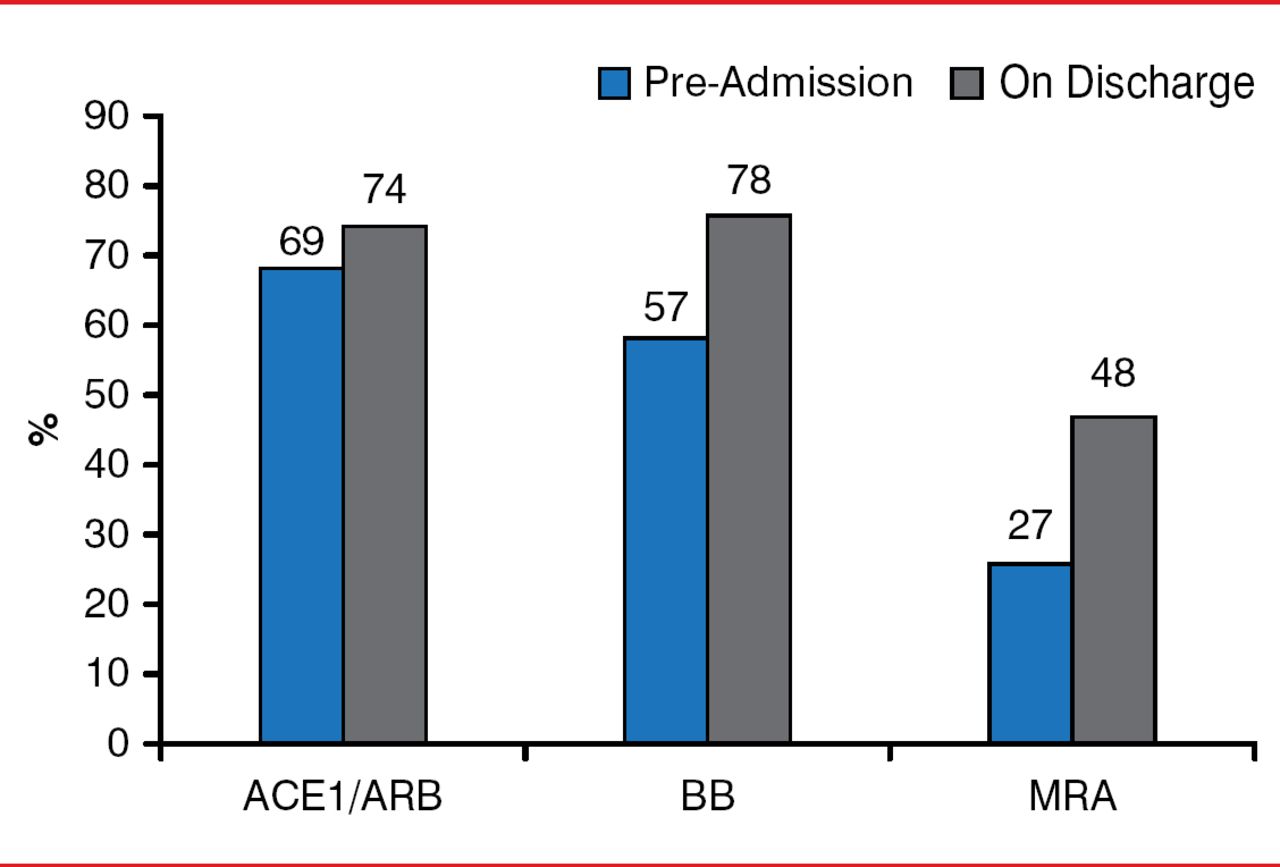
During hospitalization, 9.5% of GulfCARE patients required noninvasive ventilation, whereas 8.5% required intubation. Almost all patients (94%) were treated with diuretics; 71% received β-blockers, and 78% angiotensin-converting-enzyme inhibitors/angiotensin receptor blockers. Among patients with ADHF, there were increases in discharge medications as compared with that at pre-admission, indicative of a lack of compliance with evidence-based treatment (Figure 2).

Pre-admission and Discharge Medications among Patients with ADCHF
ACEI/ARB=angiotensin-converting-enzyme inhibitors/angiotensin receptor blockers; ADCHF=acute decompensated congestive heart failure; BB=beta-blockers; MRA=mineralocorticoid receptor antagonists.
Reproduced with permission from Sulaimab KJ, MD.
The in-hospital mortality rate was 6.3%. The etiology of HF was CAD in 54% of study participants, followed by nonischemic cardiomyopathy in 18% and hypertensive heart disease in 16% of patients. The precipitating cause of HF was acute coronary syndrome in 27% of patients and noncompliance with medications or diet in 21.7%. Most patients (89%) were discharged to home after a median hospital stay of 7 days.
Almost all patients (98.4%) were included in the 3- and 12-month follow-up examinations. Mortality was 13% at 3 months and 20% at 12 months. By 3 months, 21% of patients had been re-admitted. The number of patients receiving device therapy was low over the 12 months, as was the number of patients for whom revascularization had increased (Table 1).
Follow-up
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.