

Summary
This article reviews gout and other crystal-induced diseases, in which he reviewed important and recent publications about gout and chondrocalcinosis.
- Inflammatory Disorders
- Arthritis
- Rheumatology
Fernando Perez-Ruiz, MD, PhD, Cruces University Hospital and BioCruces Health Research Institute, Biscay, Spain, presented a year-in-review look at gout and other crystal-induced diseases, in which he reviewed important and recent publications about gout and chondrocalcinosis (CC). He briefly discussed the role of calcium pyrophosphate (CPP) in the pathogenesis of CC. The GOAL database (Genetics of Osteoarthritis and Lifestyle)—which showed low cortical bone mineral density, vascular calcification, and soft tissue calcification associated with CC—suggested a generalized constitutional predisposition to calcium crystal formation [Abhishek A et al. Ann Rheum Dis 2013]. An analysis of GOAL and the Nottingham Osteoarthritis Case-Control study supports the role of extracellular inorganic pyrophosphate in the pathogenesis of CC [Abhishek A et al. Arthritis Res Ther 2014]. A retrospective analysis showed that CPP and monosodium urate crystals can be detected more frequently than expected in synovial fluid (SF) from patients previously diagnosed with arthritis, gout, or other arthropathies, suggesting SF should be analyzed to diagnose associated comorbidities linked to the presence of crystals [Oliviero F et al. Joint Bone Spine 2013]. CPP deposits can be detected with ultrasound, radiograph, or computed tomography (CT), with the knee being the most useful joint for detection [Filippou G et al. Ann Rheum Dis 2013] and ultrasound the most sensitive modality [Barskova VG et al. Rheumatology 2013]. Currently, no publications mention treatment for CPP-associated CC.
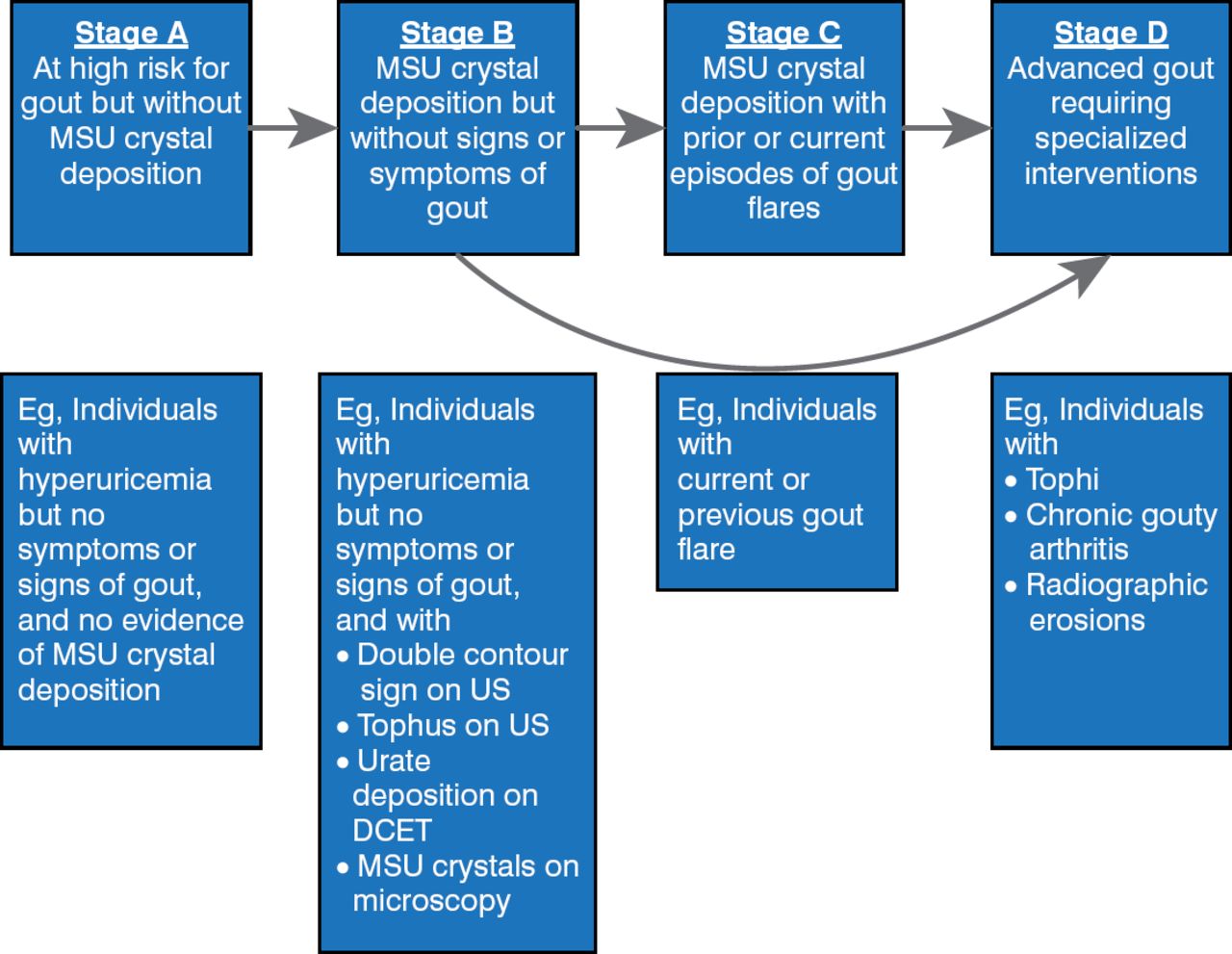
Dr. Perez-Ruiz then turned to gout, which evolves from asymptomatic hyperuricemia (>6 mg/dL) to asymptomatic urate crystal deposits in tissues and, if not treated, worsens to intermittent flares to clinical gout and, finally, to refractory gout [Bardin T, Richette P. Curr Opin Rheumatol 2014]. A revised staging system has been proposed for hyperuricemia and gout that addresses pathology in addition to symptoms [Dalbeth N, Stamp L. Ann Rheum Dis 2014]. This system is illustrated in Figure 1. Dr. Perez-Ruiz would like to see definitions of risk added to this schema, and he disagrees that the presence of tophi in Stage B would be asymptomatic.

A Proposed Revised Staging System for Hyperuricemia and Gout
DCET=dicarboxyethoxythiamine; MSU=monosodium urate; US=ultrasound.
Staging system based on the American Heart Association staging for heart failure.
Reproduced from Dalbeth N et al. Hyperuricaemia and gout: time for a new staging system? Ann Rheum Dis 2014; 0:1–3. doi:10.1136/annrheumdis-2014-20530. With permission from the BMJ Publishing Group.
Recent studies are clarifying the pathophysiology of gout. Dysfunction of ABCG2, a transporter that regulates serum uric acid levels, is associated with early-onset gout, at least in male Japanese patients [Matsuo H et al. Sci Rep 2013]. Ultrasound appears promising for diagnosis and management of gout, but further studies are needed. Dual-energy CT has been used, but it detects only dense tophi in later stages of disease [Melzer R et al. Semin Arthritis Rheum 2013] and appears most effective in detection in lower limbs [Mallinson PI et al. Skeletal Radiol 2014].
New therapies to decrease hyperuricemia are being investigated—for example, combination febuxostat plus lesinurad, which is in an early-phase trial and shows some efficacy [Fleischmann R et al. Rheumatol 2014]. Patient education has been shown in a proof-of-concept study to increase adherence to curative therapy and reduce adverse events and drug interactions [Rees F et al. Ann Rheum Dis 2013].
According to the authors, the treatment of CPP deposition disease needs further development. Current gout therapy focuses on treating episodes of acute inflammation. New treatments for gout are needed to achieve target serum uric acid levels, and lower targets should be considered to reduce crystal deposition.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.