

Summary
The aorta and its branches are involved in about 30% of patients with giant cell arteritis (GCA) [Nuenningh-off DM et al. Arthritis Rheum 2003]. Patients with GCA have a 17-fold risk for developing a thoracic aortic aneurysm and a 2.4-fold risk for developing an abdominal aneurysm [Evans JM et al. Ann Intern Med 1995]. Aortic aneurysm in GCA is poorly understood, with few data on risk and predictors of dissection and rupture. The current guidelines for monitoring and management of aortic aneurysm do not address this unique population.
- Rheumatology Clinical Trials
- Vasculitis
- Inflammatory Disorders
- Rheumatology Clinical Trials
- Vasculitis
- Inflammatory Disorders
- Rheumatology
The aorta and its branches are involved in about 30% of patients with giant cell arteritis (GCA) [Nuenninghoff DM et al. Arthritis Rheum 2003]. Patients with GCA have a 17-fold risk for developing a thoracic aortic aneurysm and a 2.4-fold risk for developing an abdominal aneurysm [Evans JM et al. Ann Intern Med 1995]. Aortic aneurysm in GCA is poorly understood, with few data on risk and predictors of dissection and rupture. The current guidelines for monitoring and management of aortic aneurysm do not address this unique population.
This retrospective study, presented by Ashima Makol, MD, Mayo Clinic, Rochester, Minnesota, USA, had 3 objectives: (1) to systematically study aortic dissection in patients with GCA with aortic aneurysms, (2) to describe the clinical features and outcomes of aortic dissection in patients with GCA, and (3) to determine the average growth rate of aortic aneurysms and identify aneurysm size associated with aortic dissection.
The study involved patients with GCA diagnosed at the Mayo Clinic between 2000 and 2012. Data were collected from the records of patients diagnosed with GCA and aortic aneurysms with aneurysm size measured on aortic imaging. Abstracted data included clinical characteristics at diagnosis of aneurysm, aortic aneurysm dimensions at diagnosis and on follow-up imaging, and clinical presentation at the time of dissection or rupture.
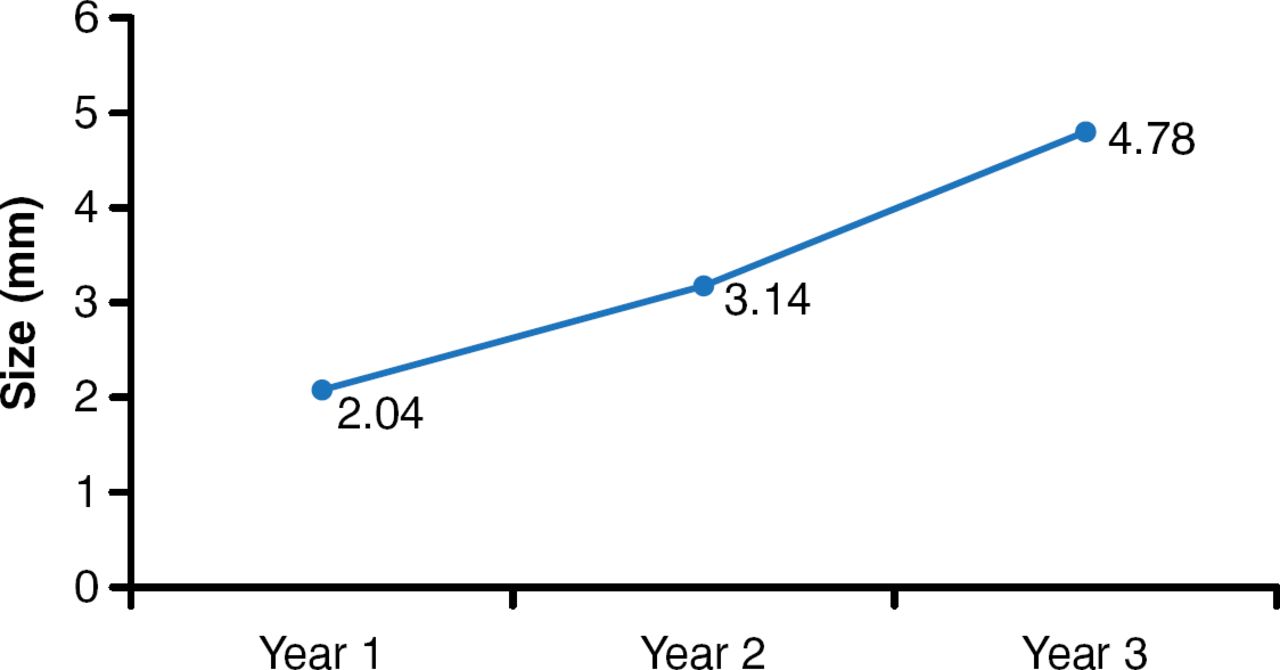
A total of 195 patients with GCA and aortic aneurysms were identified, 161 (82%) in the ascending thoracic aorta, 21 (11%) in the descending thoracic aorta, and 13 (7%) in the abdominal aorta. The mean patient age was 74 years, and 62% of patients were women. The overall mean aortic size at diagnosis was 49.3 mm. The average aneurysm overall growth rate was 1.59 mm/year for the first 3 years after diagnosis. Growth rates at 1, 2, and 3 years from baseline were 2.04, 3.14, and 4.78 mm, respectively (Figure 1).

Average Aneurysm Growth From Baseline
Reproduced with permission from A Makol, MD.
A total of 14 aortic dissections and 1 rupture were reported, all involving the thoracic aorta. The most common presenting symptoms were chest pain (75%) and syncope (18%). Patients with aortic dissection or rupture had similar characteristics to the baseline cohort. Drugs used at the time of dissection or rupture included glucocorticoids (58%), methotrexate (8%), β-blockers (83%), aspirin (67%), statins (33%), and angiotensin-converting enzyme inhibitors (50%).
The mean maximal aneurysmal dilation at the time of dissection or rupture was 54±11 mm (range, 41–80 mm). The size of the aneurysm at the last follow-up was not predictive of dissection or rupture; intact aneurysms were a mean 50±11 mm (p=0.72). There was no difference in aneurysm size at diagnosis between dissected or ruptured aneurysms (51±10 mm) and those that did not dissect or rupture (49±11 mm) (p=0.47).
Emergent surgical repair was performed in 8 of 15 patients (57%) with dissection or rupture (88% in the ascending aorta). Medical management was attempted in 7 of 15 (47%), but 4 required surgical intervention. The overall mortality rate at 30 days was 14%.
There was an 8% incidence of acute aortic syndrome in this cohort of patients with GCA. The data analysis showed that dissection can occur at any size and that aortic size at diagnosis or follow-up did not predict dissection or rupture. This study demonstrated that acute aortic syndrome in patients with GCA has a significant risk for mortality.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.